
Overview of Acute Viral Hepatitis
- Symptoms and Signs |
- Diagnosis |
- Treatment |
- Prevention |
- Key Points |
Acute viral hepatitis is diffuse liver inflammation caused by specific hepatotropic viruses that have diverse modes of transmission and epidemiologies. Although acute viral hepatitis can be asymptomatic, a nonspecific viral prodrome is often followed by anorexia, nausea, and often fever or right upper quadrant pain. Jaundice can develop, typically as other symptoms begin to resolve. Most cases resolve spontaneously, but some progress to chronic hepatitis. Occasionally, acute viral hepatitis progresses to acute liver failure (indicating fulminant hepatitis). Diagnosis is by liver tests and serologic tests to identify the virus. Good hygiene and universal precautions can prevent acute viral hepatitis. Depending on the specific virus, preexposure and postexposure prophylaxis may be possible using vaccines or serum globulins. Treatment is usually supportive.
(See also Causes of Hepatitis and Neonatal Hepatitis B Virus Infection .)
Acute viral hepatitis is a common, worldwide disease that has different causes; each type shares clinical, biochemical, and morphologic features. The term acute viral hepatitis often refers to infection of the liver by one of the hepatitis viruses. Other viruses (eg, Epstein-Barr virus , yellow fever virus , cytomegalovirus ) can also cause acute viral hepatitis but less commonly.
Etiology of Acute Viral Hepatitis
At least 5 specific viruses appear to be responsible (see table Characteristics of Hepatitis Viruses ) for acute viral hepatitis:
Hepatitis A (HAV)
Hepatitis B (HBV)
Hepatitis C (HCV)
Hepatitis D (HDV)
Hepatitis E (HEV)
Other unidentified viruses probably also cause acute viral hepatitis.
Characteristics of Hepatitis Viruses
Nucleic acid | RNA | DNA | RNA | * | RNA |
Serologic diagnosis | IgM anti-HAV | HBsAg | Anti-HCV | Anti-HDV | Anti-HEV |
Major transmission | Fecal-oral | Blood | Blood | Needle | Water |
Incubation period (days) | 15–45 | 40–180 | 20–120 | 30–180 | 14–60 |
Epidemics | Yes | No | No | No | Yes |
Chronicity | No | Yes | Yes | Yes | No |
Liver cancer | No | Yes | Yes | Yes | No |
| = IgM antibody to hepatitis A virus. | |||||
Symptoms and Signs of Acute Viral Hepatitis
Some manifestations of acute hepatitis are virus-specific (see discussions of individual hepatitis viruses) and some patients are asymptomatic, but in general, acute infection tends to develop in predictable phases:
Incubation period: The virus multiplies and spreads without causing symptoms (see table Characteristics of Hepatitis Viruses ).
Prodromal (pre-icteric) phase: Nonspecific symptoms occur; they include profound anorexia, malaise, nausea and vomiting, a newly developed distaste for cigarettes (in smokers), and often fever or right upper quadrant abdominal pain. Urticaria and arthralgias occasionally occur, especially in HBV infection.
Icteric phase: After 3 to 10 days, the urine darkens, followed by jaundice . Systemic symptoms often regress, and patients feel better despite worsening jaundice. The liver is usually enlarged and tender, but the edge of the liver remains soft and smooth. Mild splenomegaly occurs in 15 to 20% of patients. Jaundice usually peaks within 1 to 2 weeks.
Recovery phase: During this 2- to 4-week period, jaundice fades.
Appetite usually returns after the first week of symptoms. Acute viral hepatitis usually resolves spontaneously 4 to 8 weeks after symptom onset.
Anicteric hepatitis (hepatitis without jaundice) occurs more often than icteric hepatitis in patients with HCV infection and in children with HAV infection. It typically manifests as a minor flu-like illness.
Recrudescent hepatitis occurs in a few patients and is characterized by recurrent manifestations during the recovery phase.
Manifestations of cholestasis may develop during the icteric phase (called cholestatic hepatitis) but usually resolve. When they persist, they cause prolonged jaundice, elevated alkaline phosphatase, and pruritus, despite general regression of inflammation.
Diagnosis of Acute Viral Hepatitis
Liver tests (aspartate aminotransferase [AST] and alanine aminotransferase [ALT] elevated out of proportion to alkaline phosphatase, usually with hyperbilirubinemia)
Viral serologic testing
Prothrombin/international normalized ratio (PT/INR) measurement
Initial diagnosis of acute hepatitis
Acute hepatitis must first be differentiated from other disorders that cause similar symptoms. In the prodromal phase, hepatitis mimics various nonspecific viral illnesses and is difficult to diagnose. Anicteric patients suspected of having hepatitis based on risk factors are tested initially with liver tests, including aminotransferases, bilirubin, and alkaline phosphatase. Acute hepatitis often manifests in the icteric phase and so should be differentiated from other disorders causing jaundice (see figure Simplified Diagnostic Approach to Possible Acute Viral Hepatitis ).
Acute hepatitis can usually be differentiated from other causes of jaundice by
Its marked elevations of AST and ALT: Often ≥ 400 IU/L (6.68 microkat/L)
ALT is typically higher than AST, but absolute levels correlate poorly with clinical severity. Values increase early in the prodromal phase, peak before jaundice is maximal, and fall slowly during the recovery phase. Urinary bilirubin usually precedes jaundice. Hyperbilirubinemia in acute hepatitis varies in severity, and fractionation has no clinical value. Alkaline phosphatase is usually only moderately elevated; marked elevation suggests extrahepatic cholestasis and prompts imaging tests (eg, ultrasonography).
Liver biopsy is usually not needed unless the diagnosis is uncertain.
If laboratory results suggest acute hepatitis, particularly if ALT and AST are > 1000 IU/L (16.7 microkat/L), PT/INR is measured to assess liver function.
Manifestations of portosystemic encephalopathy combined with bleeding diathesis or prolongation of INR suggest acute liver failure , indicating fulminant hepatitis .
If acute hepatitis is suspected, efforts are next directed toward identifying its cause. A history of exposure may provide the only clue of drug-induced or toxic hepatitis. The history should also elicit risk factors for viral hepatitis.
Prodromal sore throat and diffuse adenopathy suggest infectious mononucleosis rather than viral hepatitis.
Simplified Diagnostic Approach to Possible Acute Viral Hepatitis
* Obtain additional laboratory studies for hepatitis A (see table ), hepatitis B (see table ), and hepatitis C (see table ). ALT = alanine aminotransferase; anti-HCV = antibody to hepatitis C virus; AST = aspartate aminotransferase; HBsAg = hepatitis B surface antigen; IgM anti-HAV = IgM antibody to hepatitis A virus. |
In patients with findings suggesting acute viral hepatitis, the following studies are done to screen for hepatitis viruses A, B, and C:
IgM antibody to HAV (IgM anti-HAV)
Hepatitis B surface antigen (HBsAg)
IgM antibody to hepatitis B core (IgM anti-HBc)
Antibody to HCV (anti-HCV)
Hepatitis C RNA (HCV-RNA) polymerase chain reaction
If any are positive, further serologic testing may be necessary to differentiate acute from past or chronic infection (see tables Hepatitis A Serology , Hepatitis B Serology , and Hepatitis C Serology ).
If serologically confirmed HBV infection is severe, anti-HDV is measured.
If the patient has recently traveled to an endemic area or is immunosuppressed, IgM antibody to HEV (IgM anti-HEV) should be measured if the test is available.
Biopsy is usually unnecessary but, if done, usually reveals similar histopathology regardless of the specific virus:
Patchy cell dropout
Acidophilic hepatocellular necrosis
Mononuclear inflammatory infiltrate
Histologic evidence of regeneration
Preservation of the reticulin framework
HBV infection can occasionally be diagnosed based on the presence of ground-glass hepatocytes (caused by HBsAg-packed cytoplasm) and using special immunologic stains for the viral components. However, these findings are unusual in acute HBV infection and are much more common in chronic HBV infection.
Treatment of Acute Viral Hepatitis
Supportive care
Treatment of acute hepatitis C, partly to prevent transmission to others
No treatments attenuate acute viral hepatitis. Alcohol should be avoided because it can increase liver damage. Restrictions on diet or activity, including commonly prescribed bed rest, have no scientific basis.
Patients with acute HCV infection should be treated with antiviral therapy upon initial diagnosis without awaiting spontaneous resolution in order to prevent transmission to others. Owing to the high efficacy and safety, the same regimens that are recommended for chronic HCV infection are recommended for acute infection ( 1 ).
Viral hepatitis should be reported to the local or state health department.
Treatment reference
1. American Association for the Study of Liver Diseases (AASLD) and Infection Diseases Society of America (IDSA) : HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Management of Acute HCV Infection. Accessed May 7, 2024.
Prevention of Acute Viral Hepatitis
Because treatments have limited efficacy, prevention of viral hepatitis is very important.
General measures
Good personal hygiene helps prevent transmission, particularly fecal-oral transmission as occurs with HAV and HEV.
Blood and other body fluids (eg, saliva, semen) of patients with acute HBV and HCV infection and stool of patients with HAV infection are considered infectious. Barrier protection is recommended, but isolation of patients does little to prevent spread of HAV and is of no value in HBV or HCV infection.
Posttransfusion infection is minimized by avoiding unnecessary transfusions and by screening all donors for hepatitis B and C. Screening has decreased the incidence of posttransfusion hepatitis B and hepatitis C, which are now extremely rare in the United States.
Immunoprophylaxis
Immunoprophylaxis can involve active immunization using vaccines and passive immunization.
Vaccines for hepatitis A and hepatitis B are available in the United States.
Routine vaccination for hepatitis A and B is recommended in the United States for all children and for adults at high risk (see Adult Immunization Schedule ).
A vaccine for hepatitis E is not available in the United States but is available in China.
No product exists for immunoprophylaxis of HCV or HDV. However, prevention of HBV infection prevents HDV infection. The propensity of HCV for changing its genome hampers vaccine development.
Transmission is the fecal-oral route for hepatitis A and E parenterally or via blood for hepatitis B and C.
Hepatitis B and C, unlike hepatitis A, predispose to chronic hepatitis and liver cancer (if chronic).
Patients with acute viral hepatitis may be anicteric or even asymptomatic.
Do viral serologic testing (IgM anti-HAV, HBsAg, anti-HCV) if clinical findings are consistent with acute viral hepatitis and AST and ALT are elevated out of proportion to alkaline phosphatase.
Treat patients supportively. Treat acute hepatitis C to prevent transmission.
Routine vaccination for hepatitis A and B is recommended in the United States for all children and for adults at high risk.

Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences

- Fact sheets
- Facts in pictures
Publications
- Questions and answers
- Tools and toolkits
- Endometriosis
- Excessive heat
- Mental disorders
- Polycystic ovary syndrome
- All countries
- Eastern Mediterranean
- South-East Asia
- Western Pacific
- Data by country
- Country presence
- Country strengthening
- Country cooperation strategies
- News releases
Feature stories
- Press conferences
- Commentaries
- Photo library
- Afghanistan
- Cholera
- Coronavirus disease (COVID-19)
- Greater Horn of Africa
- Israel and occupied Palestinian territory
- Disease Outbreak News
- Situation reports
- Weekly Epidemiological Record
- Surveillance
- Health emergency appeal
- International Health Regulations
- Independent Oversight and Advisory Committee
- Classifications
- Data collections
- Global Health Estimates
- Mortality Database
- Sustainable Development Goals
- Health Inequality Monitor
- Global Progress
- World Health Statistics
- Partnerships
- Committees and advisory groups
- Collaborating centres
- Technical teams
- Organizational structure
- Initiatives
- General Programme of Work
- WHO Academy
- Investment in WHO
- WHO Foundation
- External audit
- Financial statements
- Internal audit and investigations
- Programme Budget
- Results reports
- Governing bodies
- World Health Assembly
- Executive Board
- Member States Portal
- Health topics /
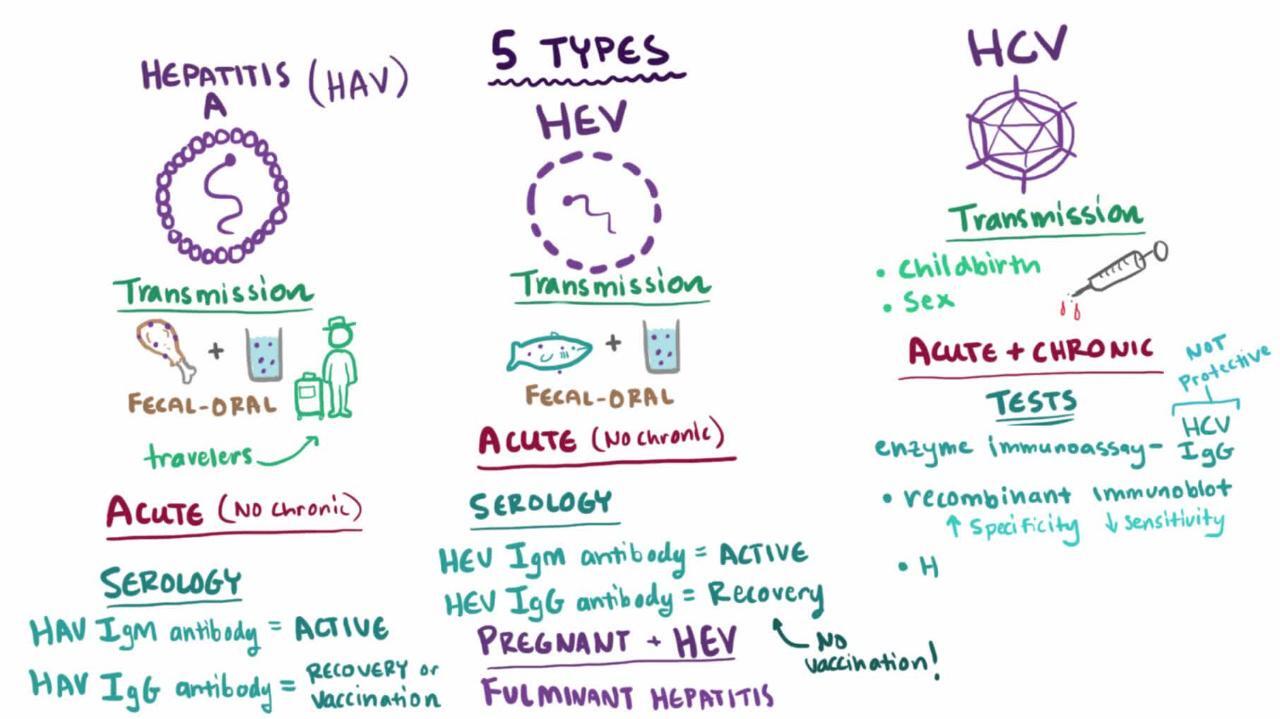
Hepatitis is an inflammation of the liver that is caused by a variety of infectious viruses and noninfectious agents leading to a range of health problems, some of which can be fatal. There are five main strains of the hepatitis virus, referred to as types A, B, C, D and E. While they all cause liver disease, they differ in important ways including modes of transmission, severity of the illness, geographical distribution and prevention methods. In particular, types B and C lead to chronic disease in hundreds of millions of people and together are the most common cause of liver cirrhosis, liver cancer and viral hepatitis-related deaths. An estimated 354 million people worldwide live with hepatitis B or C, and for most, testing and treatment remain beyond reach.
Some types of hepatitis are preventable through vaccination. A WHO study found that an estimated 4.5 million premature deaths could be prevented in low- and middle-income countries by 2030 through vaccination, diagnostic tests, medicines and education campaigns. WHO’s global hepatitis strategy, endorsed by all WHO Member States, aims to reduce new hepatitis infections by 90% and deaths by 65% between 2016 and 2030.
Many people with hepatitis A, B, C, D or E exhibit only mild symptoms or no symptoms at all. Each form of the virus, however, can cause more severe symptoms. Symptoms of hepatitis A, B and C may include fever, malaise, loss of appetite, diarrhoea, nausea, abdominal discomfort, dark-coloured urine and jaundice (a yellowing of the skin and whites of the eyes). In some cases, the virus can also cause a chronic liver infection that can later develop into cirrhosis (a scarring of the liver) or liver cancer. These patients are at risk of death.
Hepatitis D (HDV) is only found in people already infected with hepatitis B (HBV); however, the dual infection of HBV and HDV can cause a more serious infection and poorer health outcomes, including accelerated progression to cirrhosis. Development of chronic hepatitis D is rare.
Hepatitis E (HEV) begins with mild fever, reduced appetite, nausea and vomiting lasting for a few days. Some persons may also have abdominal pain, itching (without skin lesions), skin rash or joint pain. They may also exhibit jaundice, with dark urine and pale stools, and a slightly enlarged, tender liver (hepatomegaly), or occasionally acute liver failure.
Safe and effective vaccines are available to prevent hepatitis B virus (HBV). This vaccine also prevents the development of hepatitis D virus (HDV) and given at birth strongly reduces transmission risk from mother to child. Chronic hepatitis B infection can be treated with antiviral agents. Treatment can slow the progression of cirrhosis, reduce incidence of liver cancer and improve long term survival. Only a proportion of people with chronic hepatitis B infection will require treatment. A vaccine also exists to prevent infections of hepatitis E (HEV), although it is not currently widely available. There are no specific treatments for HBV and HEV and hospitalization is not usually required. It is advised to avoid unnecessary medications due to the negative effect on liver function caused by these infections.
Hepatitis C (HCV) can cause both acute and chronic infection. Some people recover on their own, while others develop a life-threatening infection or further complications, including cirrhosis or cancer. There is no vaccine for hepatitis C. Antiviral medicines can cure more than 95% of persons with hepatitis C infection, thereby reducing the risk of death from cirrhosis and liver cancer, but access to diagnosis and treatment remains low.
Hepatitis A virus (HAV) is most common is low- and middle-income countries due to reduced access to clean and reliable water sources and the increased risk of contaminated food. A safe and effective vaccine is available to prevent hepatitis A. Most HAV infections are mild, with the majority of people recovering fully and developing immunity to further infection. However, these infections can also rarely be severe and life threatening due to the risk of liver failure.
- Hepatitis A
- Hepatitis B
- Hepatitis C
- Hepatitis D
- Hepatitis E
- Immunization coverage
- What is hepatitis?
- Severe acute hepatitis of unknown cause in children
- Hepatitis B: How can I protect myself?
- Guidelines on hepatitis
- Global reporting system for hepatitis
- Acute hepatitis of unknown aetiology
- Global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections, for the period 2022–2030 (WHA75.20)
- WHA67.6: hepatitis
- WHA63.18: viral hepatitis
- Global Hepatitis Programme
WHO updates HIV testing guidance: more self-testing, integration, and prevention support
Antiretrovirals in Pregnancy Research Toolkit
WHO prequalifies the first self-test for hepatitis C virus
New report flags major increase in sexually transmitted infections, amidst challenges in HIV and hepatitis
Elimination of mother-to-child transmission of HIV and syphilis in Belize, Jamaica and Saint Vincent and the Grenadines
WHO sounds alarm on viral hepatitis infections claiming 3500 lives each day
WHO publishes new guidelines on hepatitis B
Reaching men with person-centred health services through evidence-based approaches and interventions
WHO commends Egypt for its progress on the path to eliminate hepatitis C
INFOSAN Quarterly Summary, 2023 #2
WHO launches “One life, one liver” campaign on World Hepatitis Day
Public notice and comment on new members of the Global Validation Advisory Committee (GVAC)
High-level resource mobilization conference to eliminate viral hepatitis
WHO announces the update of hepatitis B guidelines on testing and treatment
New WHO study: Making diagnosis of hepatitis C more accessible and closer to the community using point-of-care HCV viral load assays
WHO position paper on hepatitis A vaccines published
WHO publishes new guidelines on HIV, hepatitis and STIs for key populations
WHO and UNAIDS support countries to introduce virtual interventions and HIV self-testing
WHO and ANRS Emerging Infectious Diseases strengthen their collaboration in the area of HIV, viral hepatitis and sexually transmitted infections
WHO publishes updated guidance on hepatitis C infection – with new recommendations on treatment of adolescents and children, simplified service delivery and diagnostics

Implementing the global health sector strategies on HIV, viral hepatitis and sexually transmitted infections,...
This report is the first of a series of biennial progress reports on the implementation of the Global health sector strategies on, respectively, HIV, viral...

Consolidated guidelines on differentiated HIV testing services
These guidelines outline a public health approach to strengthening and expanding HIV testing services (HTS). They present and discuss key updates...

Fourth Consultation of the Regional Expert Panel for Verification of Hepatitis B Control in the South-East...
Hepatitis B control had gained momentum in the WHO South-East (SE) Asia Region as its public health burden had been recognized even prior to the COVID-19...

Recommended package of enabling and health interventions for HIV, viral hepatitis and STI prevention,...
In 2022, WHO published the Consolidated guidelines on HIV, viral hepatitis and STI prevention, diagnosis, treatment and care for key populations. These...

World Hepatitis Day 2024
It's time for action, infographics.

Deaths from viral hepatitis-related causes are increasing.

Most countries overpay for viral hepatitis medicines.

Of the 304 million people living with hepatitis B and C, only 7 million are treated for hepatitis B and 12.5 million people for hepatitis C.

Most people with chronic viral hepatitis don't realize they have it.

World Hepatitis Day 2024 – It’s time for action

WHO guidelines for key populations: what is new and what is important

Bringing hepatitis care closer to communities

Hepatitis can’t wait
Tackling health facility intersectional stigma faced by key populations in Ghana
Donors making a difference: WHO, communities and partners collaborate to end infectious diseases
Donors making a difference: the resilient spirit of women providing and receiving health care
WHO Youtube Channel

Hepatitis: WHO videos playlis
Related topics.
Sexually transmitted infections (STIs)
Universal health coverage
Masks Strongly Recommended but Not Required in Maryland, Starting Immediately
Due to the downward trend in respiratory viruses in Maryland, masking is no longer required but remains strongly recommended in Johns Hopkins Medicine clinical locations in Maryland. Read more .
- Vaccines
- Masking Guidelines
- Visitor Guidelines
Hepatitis is a general term used to describe inflammation of the liver. Liver inflammation can be caused by several viruses (viral hepatitis), chemicals, drugs, alcohol, certain genetic disorders or by an overactive immune system that mistakenly attacks the liver, called autoimmune hepatitis. Depending on its course, hepatitis can be acute, which flares up suddenly and then goes away, or chronic, which is a long-term condition usually producing more subtle symptoms and progressive liver damage.
Types of Hepatitis
There are five viruses that cause the different forms of viral hepatitis: hepatitis A, B, C, D and E. Hepatitis A is mostly a food-borne illness and can be spread through contaminated water and unwashed food. It is the easiest to transmit, especially in children, but is also the least likely to damage the liver and is usually mild and is completely resolved within six months. Hepatitis B can be transmitted through exposure to contaminated blood, needles, syringes or bodily fluids and from mother to baby. It is a chronic disorder and in some cases may lead to long-term liver damage, liver cancer and cirrhosis of the liver after many years of carrying the virus. Hepatitis C is only transmitted through infected blood or from mother to newborn during childbirth. It too can lead to liver cancer and cirrhosis in the long term. Hepatitis D is only found in people who are also infected with hepatitis B. Hepatitis E is predominantly found in Africa, Asia and South America. Certain generally safe medications can be toxic to the liver and cause hepatitis (drug-induced hepatitis) when taken in excess or in very high doses. These include acetaminophen (Tylenol) and even vitamin A. Check with your pediatrician about appropriate dosing for your child.
Autoimmune hepatitis
Hepatitis A
- Hepatitis B
- Hepatitis C
- Hepatitis D
Hepatitis E
Neonatal hepatitis
Abdominal tenderness, especially in the upper right corner
Jaundice (yellowing of the skin and the white portion of the eyes)
Dark-colored urine
Lightly colored stools
Abdominal pain
Nausea with or without vomiting
Abdominal swelling due to fluid retention
The following are required to diagnose hepatitis:
Physical exam, which may or may not reveal a swollen, enlarged liver
Blood tests to check liver enzymes that are elevated when the liver is damaged or infected, as well as blood tests to check for the presence of any of the five viruses causing hepatitis
Ultrasound of the liver to detect any changes
Liver biopsy to confirm suspected inflammation when other tests are inconclusive and to determine the exact degree of liver damage
To prevent infection, children — or anyone who has not been previously vaccinated — should be vaccinated against hepatitis B and hepatitis A. There are no vaccines against hepatitis types C, D and E. There is no cure for hepatitis once it occurs. Treatment focuses on preventing further damage to the liver, reversing existing damage if possible and symptom relief. Most cases of acute hepatitis will resolve over time. In autoimmune hepatitis, certain medications may be used to help keep the overactive immune system in check and prevent further attacks on the liver.
When to Call for Help?
If your child develops symptoms suggestive of liver inflammation, as listed above, call your pediatrician.
- Alcoholic Hepatitis
- Autoimmune Hepatitis
- Drug-Induced Hepatitis
- Hepatitis A and E
- Hepatitis in Children
- Neonatal Hepatitis
Find a Doctor
Specializing In:
- Hepatitis B (HBV)
- Hepatitis C (HCV)
- Viral Hepatitis
- Acute Viral Hepatitis
- Acute or Chronic Viral Hepatitis
Request an Appointment
Specializing In
At Another Johns Hopkins Member Hospital:
- Howard County Medical Center
- Sibley Memorial Hospital
- Suburban Hospital
Related Topics
- Infectious Diseases
Overview of Acute Viral Hepatitis
- Symptoms and Signs |
- Diagnosis |
- Treatment |
- Prevention |
- Key Points |
Acute viral hepatitis is diffuse liver inflammation caused by specific hepatotropic viruses that have diverse modes of transmission and epidemiologies. Although acute viral hepatitis can be asymptomatic, a nonspecific viral prodrome is often followed by anorexia, nausea, and often fever or right upper quadrant pain. Jaundice can develop, typically as other symptoms begin to resolve. Most cases resolve spontaneously, but some progress to chronic hepatitis. Occasionally, acute viral hepatitis progresses to acute liver failure (indicating fulminant hepatitis). Diagnosis is by liver tests and serologic tests to identify the virus. Good hygiene and universal precautions can prevent acute viral hepatitis. Depending on the specific virus, preexposure and postexposure prophylaxis may be possible using vaccines or serum globulins. Treatment is usually supportive.
(See also Causes of Hepatitis and Neonatal Hepatitis B Virus Infection .)
Acute viral hepatitis is a common, worldwide disease that has different causes; each type shares clinical, biochemical, and morphologic features. The term acute viral hepatitis often refers to infection of the liver by one of the hepatitis viruses. Other viruses (eg, Epstein-Barr virus , yellow fever virus , cytomegalovirus ) can also cause acute viral hepatitis but less commonly.
Etiology of Acute Viral Hepatitis
At least 5 specific viruses appear to be responsible (see table Characteristics of Hepatitis Viruses ) for acute viral hepatitis:
Hepatitis A (HAV)
Hepatitis B (HBV)
Hepatitis C (HCV)
Hepatitis D (HDV)
Hepatitis E (HEV)
Other unidentified viruses probably also cause acute viral hepatitis.
Characteristics of Hepatitis Viruses
Nucleic acid | RNA | DNA | RNA | * | RNA |
Serologic diagnosis | IgM anti-HAV | HBsAg | Anti-HCV | Anti-HDV | Anti-HEV |
Major transmission | Fecal-oral | Blood | Blood | Needle | Water |
Incubation period (days) | 15–45 | 40–180 | 20–120 | 30–180 | 14–60 |
Epidemics | Yes | No | No | No | Yes |
Chronicity | No | Yes | Yes | Yes | No |
Liver cancer | No | Yes | Yes | Yes | No |
| = IgM antibody to hepatitis A virus. | |||||
Symptoms and Signs of Acute Viral Hepatitis
Some manifestations of acute hepatitis are virus-specific (see discussions of individual hepatitis viruses) and some patients are asymptomatic, but in general, acute infection tends to develop in predictable phases:
Incubation period: The virus multiplies and spreads without causing symptoms (see table Characteristics of Hepatitis Viruses ).
Prodromal (pre-icteric) phase: Nonspecific symptoms occur; they include profound anorexia, malaise, nausea and vomiting, a newly developed distaste for cigarettes (in smokers), and often fever or right upper quadrant abdominal pain. Urticaria and arthralgias occasionally occur, especially in HBV infection.
Icteric phase: After 3 to 10 days, the urine darkens, followed by jaundice . Systemic symptoms often regress, and patients feel better despite worsening jaundice. The liver is usually enlarged and tender, but the edge of the liver remains soft and smooth. Mild splenomegaly occurs in 15 to 20% of patients. Jaundice usually peaks within 1 to 2 weeks.
Recovery phase: During this 2- to 4-week period, jaundice fades.
Appetite usually returns after the first week of symptoms. Acute viral hepatitis usually resolves spontaneously 4 to 8 weeks after symptom onset.
Anicteric hepatitis (hepatitis without jaundice) occurs more often than icteric hepatitis in patients with HCV infection and in children with HAV infection. It typically manifests as a minor flu-like illness.
Recrudescent hepatitis occurs in a few patients and is characterized by recurrent manifestations during the recovery phase.
Manifestations of cholestasis may develop during the icteric phase (called cholestatic hepatitis) but usually resolve. When they persist, they cause prolonged jaundice, elevated alkaline phosphatase, and pruritus, despite general regression of inflammation.
Diagnosis of Acute Viral Hepatitis
Liver tests (aspartate aminotransferase [AST] and alanine aminotransferase [ALT] elevated out of proportion to alkaline phosphatase, usually with hyperbilirubinemia)
Viral serologic testing
Prothrombin/international normalized ratio (PT/INR) measurement
Initial diagnosis of acute hepatitis
Acute hepatitis must first be differentiated from other disorders that cause similar symptoms. In the prodromal phase, hepatitis mimics various nonspecific viral illnesses and is difficult to diagnose. Anicteric patients suspected of having hepatitis based on risk factors are tested initially with liver tests, including aminotransferases, bilirubin, and alkaline phosphatase. Acute hepatitis often manifests in the icteric phase and so should be differentiated from other disorders causing jaundice (see figure Simplified Diagnostic Approach to Possible Acute Viral Hepatitis ).
Acute hepatitis can usually be differentiated from other causes of jaundice by
Its marked elevations of AST and ALT: Often ≥ 400 IU/L (6.68 microkat/L)
ALT is typically higher than AST, but absolute levels correlate poorly with clinical severity. Values increase early in the prodromal phase, peak before jaundice is maximal, and fall slowly during the recovery phase. Urinary bilirubin usually precedes jaundice. Hyperbilirubinemia in acute hepatitis varies in severity, and fractionation has no clinical value. Alkaline phosphatase is usually only moderately elevated; marked elevation suggests extrahepatic cholestasis and prompts imaging tests (eg, ultrasonography).
Liver biopsy is usually not needed unless the diagnosis is uncertain.
If laboratory results suggest acute hepatitis, particularly if ALT and AST are > 1000 IU/L (16.7 microkat/L), PT/INR is measured to assess liver function.
Manifestations of portosystemic encephalopathy combined with bleeding diathesis or prolongation of INR suggest acute liver failure , indicating fulminant hepatitis .
If acute hepatitis is suspected, efforts are next directed toward identifying its cause. A history of exposure may provide the only clue of drug-induced or toxic hepatitis. The history should also elicit risk factors for viral hepatitis.
Prodromal sore throat and diffuse adenopathy suggest infectious mononucleosis rather than viral hepatitis.
Simplified Diagnostic Approach to Possible Acute Viral Hepatitis
* Obtain additional laboratory studies for hepatitis A (see table ), hepatitis B (see table ), and hepatitis C (see table ). ALT = alanine aminotransferase; anti-HCV = antibody to hepatitis C virus; AST = aspartate aminotransferase; HBsAg = hepatitis B surface antigen; IgM anti-HAV = IgM antibody to hepatitis A virus. |
In patients with findings suggesting acute viral hepatitis, the following studies are done to screen for hepatitis viruses A, B, and C:
IgM antibody to HAV (IgM anti-HAV)
Hepatitis B surface antigen (HBsAg)
IgM antibody to hepatitis B core (IgM anti-HBc)
Antibody to HCV (anti-HCV)
Hepatitis C RNA (HCV-RNA) polymerase chain reaction
If any are positive, further serologic testing may be necessary to differentiate acute from past or chronic infection (see tables Hepatitis A Serology , Hepatitis B Serology , and Hepatitis C Serology ).
If serologically confirmed HBV infection is severe, anti-HDV is measured.
If the patient has recently traveled to an endemic area or is immunosuppressed, IgM antibody to HEV (IgM anti-HEV) should be measured if the test is available.
Biopsy is usually unnecessary but, if done, usually reveals similar histopathology regardless of the specific virus:
Patchy cell dropout
Acidophilic hepatocellular necrosis
Mononuclear inflammatory infiltrate
Histologic evidence of regeneration
Preservation of the reticulin framework
HBV infection can occasionally be diagnosed based on the presence of ground-glass hepatocytes (caused by HBsAg-packed cytoplasm) and using special immunologic stains for the viral components. However, these findings are unusual in acute HBV infection and are much more common in chronic HBV infection.
Treatment of Acute Viral Hepatitis
Supportive care
Treatment of acute hepatitis C, partly to prevent transmission to others
No treatments attenuate acute viral hepatitis. Alcohol should be avoided because it can increase liver damage. Restrictions on diet or activity, including commonly prescribed bed rest, have no scientific basis.
Patients with acute HCV infection should be treated with antiviral therapy upon initial diagnosis without awaiting spontaneous resolution in order to prevent transmission to others. Owing to the high efficacy and safety, the same regimens that are recommended for chronic HCV infection are recommended for acute infection ( 1 ).
Viral hepatitis should be reported to the local or state health department.
Treatment reference
1. American Association for the Study of Liver Diseases (AASLD) and Infection Diseases Society of America (IDSA) : HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Management of Acute HCV Infection. Accessed May 7, 2024.
Prevention of Acute Viral Hepatitis
Because treatments have limited efficacy, prevention of viral hepatitis is very important.
General measures
Good personal hygiene helps prevent transmission, particularly fecal-oral transmission as occurs with HAV and HEV.
Blood and other body fluids (eg, saliva, semen) of patients with acute HBV and HCV infection and stool of patients with HAV infection are considered infectious. Barrier protection is recommended, but isolation of patients does little to prevent spread of HAV and is of no value in HBV or HCV infection.
Posttransfusion infection is minimized by avoiding unnecessary transfusions and by screening all donors for hepatitis B and C. Screening has decreased the incidence of posttransfusion hepatitis B and hepatitis C, which are now extremely rare in the United States.
Immunoprophylaxis
Immunoprophylaxis can involve active immunization using vaccines and passive immunization.
Vaccines for hepatitis A and hepatitis B are available in the United States.
Routine vaccination for hepatitis A and B is recommended in the United States for all children and for adults at high risk (see Adult Immunization Schedule ).
A vaccine for hepatitis E is not available in the United States but is available in China.
No product exists for immunoprophylaxis of HCV or HDV. However, prevention of HBV infection prevents HDV infection. The propensity of HCV for changing its genome hampers vaccine development.
Transmission is the fecal-oral route for hepatitis A and E parenterally or via blood for hepatitis B and C.
Hepatitis B and C, unlike hepatitis A, predispose to chronic hepatitis and liver cancer (if chronic).
Patients with acute viral hepatitis may be anicteric or even asymptomatic.
Do viral serologic testing (IgM anti-HAV, HBsAg, anti-HCV) if clinical findings are consistent with acute viral hepatitis and AST and ALT are elevated out of proportion to alkaline phosphatase.
Treat patients supportively. Treat acute hepatitis C to prevent transmission.
Routine vaccination for hepatitis A and B is recommended in the United States for all children and for adults at high risk.
Copyright © 2024 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
- Cookie Preferences
A .gov website belongs to an official government organization in the United States.
A lock ( ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
- Hepatitis A Outbreak
- Vaccination
- Tools and Resources
- Clinical Overview
- Clinical Signs and Symptoms
- Clinical Testing and Diagnosis
- Clinical Care and Treatment
- Vaccine Administration
Related Topics:
- View All Home
- Viral Hepatitis
- Hepatitis B
- Hepatitis C
- Viral Hepatitis Statistics & Surveillance
Clinical Signs and Symptoms of Hepatitis A
- Most people who get hepatitis A have a mild, short-term illness.
- Adults are more likely than children to have symptomatic HAV infection.
- Clinicians should conduct serologic testing on patients if they have signs or symptoms consistent with HAV infection.
- CDC does not recommend routine hepatitis A screening.

Disease presentation
Older children and adults with HAV infection will typically experience symptoms.
Most (70%) of infections in children younger than age 6 are not accompanied by symptoms. When symptoms are present, young children typically do not have jaundice; most (>70%) older children and adults with HAV infection have jaundice. 1 2
Among symptomatic patients, 10%–15% might experience prolonged or relapsing symptoms up to 6 months after they become infected. 1 3 4 5 6
Incubation period
The average incubation period for HAV is 28 days (range: 15–50 days). 3 4 5
Virus survival
Depending on the environmental conditions, the virus can live outside the body for months. 6
For the public
Common symptoms.
Hepatitis A symptoms, which usually last less than 2 months, occur abruptly, and can include:
- Abdominal pain, nausea, and/or vomiting
- Dark urine or clay-colored stools
- Loss of appetite
For detailed guidance on clinical care and treatment for hepatitis A, keep reading .
Clinical assessment
Clinicians should conduct serologic testing on patients if they have signs or symptoms consistent with HAV infection and/or if they think they may have been infected with HAV. CDC does not recommend routine hepatitis A screening.
- Wasley A, Fiore A, Bell BP. Hepatitis A in the era of vaccination . Epidemiol Rev 2006;28:101–11. Epub 2006 Jun 14. Review.
- Schiff ER. Atypical clinical manifestations of hepatitis A . Vaccine 1992;10 Suppl 1:S18.
- Halliday ML, Kang LY, Zhou TK, et al. An epidemic of hepatitis A attributable to the ingestion of raw clams in Shanghai, China . J Infect Dis 1991;164(5):852–9.
- Neefe JR, Gellis SS, Stokes J Jr. Homologous serum hepatitis and infectious (epidemic) hepatitis: studies in volunteers bearing on immunological and other characteristics of the etiological agents . Am J Med 1946;1:3–22.
- Krugman S, Giles JP, Hammond J. Infectious hepatitis: Evidence for two distinctive clinical, epidemiological, and immunological types of infection . JAMA 1967;200(5):365–73.
- Abad FX, Pinto RM, Bosch A. Survival of enteric viruses on environmental fomites . Appl Environ Microbiol 1994;60(10):3704–10.
Hepatitis A
Learn more about hepatitis A, a liver disease caused by the hepatitis A virus (HAV). Find HAV information for the public and health professionals.
For Everyone
Health care providers.
Hepatitis B Clinical Presentation
- Author: Nikolaos T Pyrsopoulos, MD, PhD, MBA, FACP, AGAF, FAASLD, FRCP(Edin); Chief Editor: BS Anand, MD more...
- Sections Hepatitis B
- Practice Essentials
- Pathophysiology
- Epidemiology
- Patient Education
- Physical Examination
- Approach Considerations
- Diagnostic Tests
- Radiologic Studies
- Liver Biopsy and Histologic Features
- Pharmacologic Management
- Surgical Intervention
- Hepatitis B and Pregnancy
- Vaccination
- Long-Term Monitoring
- 2016 and 2018 AASLD Guidelines
- 2017 and 2018 EASL Recommendations
- 2015 and 2020 WHO Guidelines Summary
- Medication Summary
- Interferons
- Antihepadnaviral, Reverse Transcriptase inhibitors
- Vaccines, Inactivated, Viral
- Questions & Answers
- Media Gallery
Inquire into patients’ sexual history, occupational history, illicit drug use, and any contacts with known infection.
The spectrum of the symptomatology of hepatitis B disease varies from subclinical hepatitis to icteric hepatitis to fulminant, acute, and subacute hepatitis during the acute phase, and from an asymptomatic chronic infection state to chronic hepatitis, cirrhosis, and hepatocellular carcinoma (HCC) during the chronic phase.
Papular acrodermatitis, also recognized as Gianotti-Crosti syndrome , has been associated with hepatitis B, most commonly in children with acute infection. [ 40 ]
The following multisystem manifestations may occur in hepatitis B virus (HBV) infection:
Pleural effusion and hepatopulmonary and portopulmonary syndrome may occur in patients with cirrhosis
Diffuse intravascular coagulation may occur in patients with fulminant hepatitis
Myocarditis, pericarditis, and arrhythmia occur primarily in patients with fulminant hepatitis
Arthralgias and arthritic (serum sickness) subcutaneous nodules may also occur, but these are rare
Guillain-Barre syndrome , encephalitis, aseptic meningitis, and mononeuritis multiplex may occur in patients with acute hepatitis B
Pancreatitis may develop
Aplastic anemia is uncommon, and agranulocytosis is extremely uncommon
A variety of cutaneous manifestations have been recognized during the early course of viral hepatitis, including hives and a fleeting maculopapular rash. These various lesions are episodic, palpable, and, at times, pruritic. A discoloration of the skin can be identified after the resolution of the exanthem, particularly on the lower extremities. Women are more prone to developing cutaneous manifestations.
Acute phase
The incubation period is 1-6 months in the acute phase of hepatitis B infection. Anicteric hepatitis is the predominant form of expression for this disease. The majority of the patients are asymptomatic, but patients with anicteric hepatitis have a greater tendency to develop chronic hepatitis. Patients with symptomatology have the same symptoms as patients who develop icteric hepatitis.
Icteric hepatitis is associated with a prodromal period, during which a serum sickness –like syndrome can occur. The symptomatology is more constitutional and includes the following:
Low-grade fever
Fatigability
Disordered gustatory acuity and smell sensations (aversion to food and cigarettes)
Right upper quadrant and epigastric pain (intermittent, mild to moderate)
Patients with fulminant and subfulminant hepatitis may present with the following:
Hepatic encephalopathy
Disturbances in sleep pattern
Mental confusion
Gastrointestinal (GI) bleeding
Coagulopathy
Chronic phase
Patients with chronic hepatitis B disease can be immune tolerant or have an inactive chronic infection without any evidence of active disease. These patients are generally asymptomatic.
Patients with chronic active hepatitis, especially during the replicative state, may complain of symptomatology such as the following:
Symptoms similar to those of acute hepatitis
Mild upper quadrant pain or discomfort
If progressive liver disease is present, the following symptomatology may be present:
Hepatic decompensation
GI bleeding
The physical examination findings in hepatitis B disease vary from minimal to impressive (in patients with hepatic decompensation), according to the stage of disease.
Patients with acute hepatitis usually do not have any clinical findings, but the physical examination can reveal the following:
Jaundice (10 days after appearance of constitutional symptomatology, lasting for 1-3 mo)
Hepatomegaly (mildly enlarged, soft liver)
Splenomegaly (5-15%)
Palmar erythema (rarely)
Spider nevi (rarely)
The physical examination of patients with chronic hepatitis B virus (HBV) infection can reveal stigmata of chronic liver disease such as the following:
Hepatomegaly
Splenomegaly
Muscle wasting
Palmar erythema
Spider angioma
Vasculitis (rarely)
Patients with cirrhosis may have the following findings:
History of variceal bleeding
Peripheral edema
Gynecomastia
Testicular atrophy
Abdominal collateral veins (caput medusa)
Centers for Disease Control and Prevention. Hepatitis B information for health professionals: hepatitis B FAQs for health professionals. https://www.cdc.gov/hepatitis/HBV/index.htm. Available at https://www.cdc.gov/hepatitis/HBV/index.htm . Updated May 31, 2015; Accessed: May 23, 2017.
Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference Statement: management of hepatitis B. Ann Intern Med . 2009 Jan 20. 150(2):104-10. [QxMD MEDLINE Link] . [Full Text] .
Nguyen MH, Wong G, Gane E, Kao JH, Dusheiko G. Hepatitis B virus: advances in prevention, diagnosis, and therapy. Clin Microbiol Rev . 2020 Mar 18. 33(2):e2128652. [QxMD MEDLINE Link] . [Full Text] .
World Health Organization. Hepatitis B. July 27, 2021. Available at https://www.who.int/news-room/fact-sheets/detail/hepatitis-b . Accessed: December 2, 2021.
McMahon BJ, Holck P, Bulkow L, Snowball M. Serologic and clinical outcomes of 1536 Alaska Natives chronically infected with hepatitis B virus. Ann Intern Med . 2001 Nov 6. 135(9):759-68. [QxMD MEDLINE Link] .
Chang MH, Chen CJ, Lai MS, et al. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N Engl J Med . 1997 Jun 26. 336(26):1855-9. [QxMD MEDLINE Link] .
Fattovich G, Giustina G, Schalm SW, et al. Occurrence of hepatocellular carcinoma and decompensation in western European patients with cirrhosis type B. The EUROHEP Study Group on Hepatitis B Virus and Cirrhosis. Hepatology . 1995 Jan. 21(1):77-82. [QxMD MEDLINE Link] .
Yu MC, Yuan JM, Ross RK, Govindarajan S. Presence of antibodies to the hepatitis B surface antigen is associated with an excess risk for hepatocellular carcinoma among non-Asians in Los Angeles County, California. Hepatology . 1997 Jan. 25(1):226-8. [QxMD MEDLINE Link] .
Yang HI, Yeh SH, Chen PJ, et al. Associations between hepatitis B virus genotype and mutants and the risk of hepatocellular carcinoma. J Natl Cancer Inst . 2008 Aug 20. 100(16):1134-43. [QxMD MEDLINE Link] . [Full Text] .
Te HS, Jensen DM. Epidemiology of hepatitis B and C viruses: a global overview. Clin Liver Dis . 2010 Feb. 14(1):1-21, vii. [QxMD MEDLINE Link] .
World Health Organization. Weekly epidemiological record (WER): global routine vaccination coverage. 2011;86(46):509-20. Available at https://www.who.int/wer/2011/wer8646/en/index.html . Accessed: June 13, 2013.
Blumberg BS. Australia antigen and the biology of hepatitis B. Science . 1977 Jul 1. 197(4298):17-25. [QxMD MEDLINE Link] .
Norder H, Courouce AM, Magnius LO. Complete genomes, phylogenetic relatedness, and structural proteins of six strains of the hepatitis B virus, four of which represent two new genotypes. Virology . 1994 Feb. 198(2):489-503. [QxMD MEDLINE Link] .
Lau JY, Wright TL. Molecular virology and pathogenesis of hepatitis B. Lancet . 1993 Nov 27. 342(8883):1335-40. [QxMD MEDLINE Link] .
Chisari FV, Ferrari C. Hepatitis B virus immunopathology. Springer Semin Immunopathol . 1995. 17(2-3):261-81. [QxMD MEDLINE Link] .
Davies SE, Portmann BC, O'Grady JG, et al. Hepatic histological findings after transplantation for chronic hepatitis B virus infection, including a unique pattern of fibrosing cholestatic hepatitis. Hepatology . 1991 Jan. 13(1):150-7. [QxMD MEDLINE Link] .
Kahila Bar-Gal G, Kim MJ, Klein A, et al. Tracing hepatitis B virus to the 16th century in a Korean mummy. Hepatology . 2012 Nov. 56(5):1671-80. [QxMD MEDLINE Link] .
Gish RG, Locarnini S. Chronic hepatitis B viral infection. Yamada T, ed. Textbook of Gastroenterology . 5th ed. Oxford, UK: Blackwell Publishing; 2009. 2112-38.
Azmi AN, Tan SS, Mohamed R. Practical approach in hepatitis B e antigen-negative individuals to identify treatment candidates. World J Gastroenterol . 2014 Sep 14. 20(34):12045-55. [QxMD MEDLINE Link] . [Full Text] .
Jung MC, Diepolder HM, Pape GR. T cell recognition of hepatitis B and C viral antigens. Eur J Clin Invest . 1994 Oct. 24(10):641-50. [QxMD MEDLINE Link] .
Chisari FV. Cytotoxic T cells and viral hepatitis. J Clin Invest . 1997 Apr 1. 99(7):1472-7. [QxMD MEDLINE Link] . [Full Text] .
Kuo A, Gish R. Chronic hepatitis B infection. Clin Liver Dis . 2012 May. 16(2):347-69. [QxMD MEDLINE Link] .
Tong W, He J, Sun L, He S, Qi Q. Hepatitis B virus with a proposed genotype I was found in Sichuan Province, China. J Med Virol . 2012 Jun. 84(6):866-70. [QxMD MEDLINE Link] .
Sonneveld MJ, Rijckborst V, Zeuzem S, et al. Presence of precore and core promoter mutants limits the probability of response to peginterferon in hepatitis B e antigen-positive chronic hepatitis B. Hepatology . 2012 Jul. 56(1):67-75. [QxMD MEDLINE Link] .
Fattovich G, Giustina G, Christensen E, et al. Influence of hepatitis delta virus infection on morbidity and mortality in compensated cirrhosis type B. The European Concerted Action on Viral Hepatitis (Eurohep). Gut . 2000 Mar. 46(3):420-6. [QxMD MEDLINE Link] . [Full Text] .
Wursthorn K, Manns MP, Wedemeyer H. Natural history: the importance of viral load, liver damage and HCC. Best Pract Res Clin Gastroenterol . 2008. 22(6):1063-79. [QxMD MEDLINE Link] .
Heidrich B, Serrano BC, Idilman R, et al. HBeAg-positive hepatitis delta: virological patterns and clinical long-term outcome. Liver Int . 2012 Oct. 32(9):1415-25. [QxMD MEDLINE Link] .
Wang J, Zhao W, Cheng L, et al. CD137-mediated pathogenesis from chronic hepatitis to hepatocellular carcinoma in hepatitis B virus-transgenic mice. J Immunol . 2010 Dec 15. 185(12):7654-62. [QxMD MEDLINE Link] . [Full Text] .
Thursz MR, Thomas HC, Greenwood BM, Hill AV. Heterozygote advantage for HLA class-II type in hepatitis B virus infection. Nat Genet . 1997 Sep. 17(1):11-2. [QxMD MEDLINE Link] .
Jouanguy E, Lamhamedi-Cherradi S, Altare F, et al. Partial interferon-gamma receptor 1 deficiency in a child with tuberculoid bacillus Calmette-Guérin infection and a sibling with clinical tuberculosis. J Clin Invest . 1997 Dec 1. 100(11):2658-64. [QxMD MEDLINE Link] . [Full Text] .
Zhou J, Chen DQ, Poon VK, et al. A regulatory polymorphism in interferon-gamma receptor 1 promoter is associated with the susceptibility to chronic hepatitis B virus infection. Immunogenetics . 2009 Jun. 61(6):423-30. [QxMD MEDLINE Link] .
Frodsham AJ, Zhang L, Dumpis U, et al. Class II cytokine receptor gene cluster is a major locus for hepatitis B persistence. Proc Natl Acad Sci U S A . 2006 Jun 13. 103(24):9148-53. [QxMD MEDLINE Link] . [Full Text] .
Alper CA, Kruskall MS, Marcus-Bagley D, et al. Genetic prediction of nonresponse to hepatitis B vaccine. N Engl J Med . 1989 Sep 14. 321(11):708-12. [QxMD MEDLINE Link] .
Davila S, Froeling FE, Tan A, et al. New genetic associations detected in a host response study to hepatitis B vaccine. Genes Immun . 2010 Apr. 11(3):232-8. [QxMD MEDLINE Link] .
[Guideline] Kowdley KV, Wang CC, Welch S, Roberts H, Brosgart CL. Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology . 2012 Aug. 56(2):422-33. [QxMD MEDLINE Link] .
Tripathi N, Mousa OY. Hepatitis B. StatPearls [Internet] . 2021 Jul 18. [QxMD MEDLINE Link] . [Full Text] .
Xie WY, Sun C, He H, Deng C, Sheng Y. Estimates of the prevalence of occult HBV infection in Asia: a systematic review and meta-analysis. Infect Dis (Lond) . 2022 Dec. 54 (12):881-96. [QxMD MEDLINE Link] .
Kim BK, Han KH, Ahn SH. Prevention of hepatocellular carcinoma in patients with chronic hepatitis B virus infection. Oncology . 2011. 81 Suppl 1:41-9. [QxMD MEDLINE Link] .
Han YF, Zhao J, Ma LY, et al. Factors predicting occurrence and prognosis of hepatitis-B-virus-related hepatocellular carcinoma. World J Gastroenterol . 2011 Oct 14. 17(38):4258-70. [QxMD MEDLINE Link] . [Full Text] .
Caputo R, Gelmetti C, Ermacora E, Gianni E, Silvestri A. Gianotti-Crosti syndrome: a retrospective analysis of 308 cases. J Am Acad Dermatol . 1992 Feb. 26(2 Pt 1):207-10. [QxMD MEDLINE Link] .
[Guideline] Terrault NA, Bzowej NH, Chang KM, et al, for the American Association for the Study of Liver Diseases. AASLD guidelines for treatment of chronic hepatitis B. Hepatology . 2016 Jan. 63(1):261-83. [QxMD MEDLINE Link] . [Full Text] .
Arora S, Martin CL, Herbert M. Myth: interpretation of a single ammonia level in patients with chronic liver disease can confirm or rule out hepatic encephalopathy. CJEM . 2006 Nov. 8(6):433-5. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] Centers for Disease Control and Prevention. 2015 Sexually transmitted diseases treatment guidelines. Viral hepatitis. Centers for Disease Control and Prevention. Available at https://www.cdc.gov/std/tg2015/hepatitis.htm . June 4, 2015; Accessed: May 26, 2017.
Finnish Medical Society Duodecim. Viral hepatitis. EBM Guidelines. Evidence-Based Medicine [Internet] . Helsinki, Finland: Wiley Interscience; 2008.
New York State Department of Health. Hepatitis B virus. New York, NY: New York State Department of Health; 2008. Available at https://guideline.gov/content.aspx?id=12812 . Accessed: June 13, 2013.
[Guideline] U.S. Preventive Services Task Force. Hepatitis B virus infection in adolescents and adults: screening. December 15, 2020. Available at https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/hepatitis-b-virus-infection-screening . Accessed: December 2, 2021.
Barclay L. USPSTF shifts course, favors hepatitis B screening. Medscape Medical News. Available at https://www.medscape.com/viewarticle/825948 . May 30, 2014; Accessed: June 2, 2014.
LeFevre ML, U.S. Preventive Services Task Force. Screening for hepatitis B virus infection in nonpregnant adolescents and adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med . 2014 Jul 1. 161(1):58-66. [QxMD MEDLINE Link] .
Chou R, Dana T, Bougatsos C, Blazina I, Khangura J, Zakher B. Screening for hepatitis B virus infection in adolescents and adults: a systematic review to update the U.S. Preventive Services Task Force recommendation. Ann Intern Med . 2014 Jul 1. 161(1):31-45. [QxMD MEDLINE Link] .
Rajbhandari R, Chung RT. Screening for hepatitis B virus infection: a public health imperative. Ann Intern Med . 2014 Jul 1. 161(1):76-7. [QxMD MEDLINE Link] .
Eckman MH, Kaiser TE, Sherman KE. The cost-effectiveness of screening for chronic hepatitis B infection in the United States. Clin Infect Dis . 2011 Jun. 52(11):1294-306. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology . 2018 Apr. 67 (4):1560-99. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] Centers for Disease Control and Prevention. Testing recommendations for hepatitis C virus infection. July 29, 2020. Available at https://www.cdc.gov/hepatitis/hcv/guidelinesc.htm . Accessed: December 2, 2021.
Trinchet JC, Chaffaut C, Bourcier V, et al. Ultrasonographic surveillance of hepatocellular carcinoma in cirrhosis: a randomized trial comparing 3- and 6-month periodicities. Hepatology . 2011 Dec. 54(6):1987-97. [QxMD MEDLINE Link] .
US Food and Drug Administration. 510(k) Premarket notification: Hepatiq. Available at https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K142891 . Accessed: January 11, 2015.
Business Wire. FDA clears Hepatiq [press release]. Hepatiq: Hepatic Quantitation. Available at https://www.hepatiq.com/fdaclearshepatiq.html . Accessed: January 11, 2015.
National Institute of Diabetes and Digestive and Kidney Diseases. HALT-C (Hepatitis C Antiviral Long-term Treatment against Cirrhosis) trial website. Available at https://archives.niddk.nih.gov/haltctrial/displaypage.aspx?pagename=haltctrial/index.htm . Accessed: January 11, 2015.
Srinivasa Babu A, Wells ML, Teytelboym OM, et al. Elastography in chronic liver disease: modalities, techniques, limitations, and future directions. Radiographics . 2016 Nov-Dec. 36(7):1987-2006. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] World Health Organization. Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection. Geneva, Switzerland; WHO. 2015 Mar. [QxMD MEDLINE Link] . [Full Text] .
Nebbia G, Peppa D, Maini MK. Hepatitis B infection: current concepts and future challenges. QJM . 2012 Feb. 105(2):109-13. [QxMD MEDLINE Link] . [Full Text] .
Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology . 2009 Sep. 50(3):661-2. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] Papatheodoridis G, Buti M, Cornberg M, et al, for the European Association for the Study of the Liver. EASL clinical practice guidelines: Management of chronic hepatitis B virus infection. J Hepatol . 2012 Jul. 57(1):167-85. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] Liaw YF, Leung N, Kao JH, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int . 2008 Sep. 2(3):263-83. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] Sherman M, Shafran S, Burak K, et al. Management of chronic hepatitis B: consensus guidelines. Can J Gastroenterol . 2007 Jun. 21 Suppl C:5C-24C. [QxMD MEDLINE Link] . [Full Text] .
[Guideline] Kennedy PT, Lee HC, Jeyalingam L, et al. NICE guidelines and a treatment algorithm for the management of chronic hepatitis B: a review of 12 years experience in west London. Antivir Ther . 2008. 13(8):1067-76. [QxMD MEDLINE Link] .
Keeffe EB, Dieterich DT, Han SH, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: an update. Clin Gastroenterol Hepatol . 2006 Aug. 4(8):936-62. [QxMD MEDLINE Link] .
New York State Department of Health. Prevention of secondary disease: preventive medicine. Viral hepatitis. New York, NY: New York State Department of Health; 2010. Available at https://guideline.gov/content.aspx?id=24043 . Accessed: June 13, 2013.
Pharmasset voluntarily halts clinical studies with clevudine in hepatitis B infected patients. Medical News Today. Available at https://www.medicalnewstoday.com/releases/146749.php . April 21, 2009; Accessed: June 13, 2013.
Mutimer D, Naoumov N, Honkoop P, et al. Combination alpha-interferon and lamivudine therapy for alpha-interferon-resistant chronic hepatitis B infection: results of a pilot study. J Hepatol . 1998 Jun. 28(6):923-9. [QxMD MEDLINE Link] .
Gara N, Zhao X, Collins MT, et al. Renal tubular dysfunction during long-term adefovir or tenofovir therapy in chronic hepatitis B. Aliment Pharmacol Ther . 2012 Jun. 35(11):1317-25. [QxMD MEDLINE Link] . [Full Text] .
Lange CM, Bojunga J, Hofmann WP, et al. Severe lactic acidosis during treatment of chronic hepatitis B with entecavir in patients with impaired liver function. Hepatology . 2009 Dec. 50(6):2001-6. [QxMD MEDLINE Link] .
Wong DK, Cheung AM, O'Rourke K, Naylor CD, Detsky AS, Heathcote J. Effect of alpha-interferon treatment in patients with hepatitis B e antigen-positive chronic hepatitis B. A meta-analysis. Ann Intern Med . 1993 Aug 15. 119(4):312-23. [QxMD MEDLINE Link] .
Tseng TC, Liu CJ, Su TH, et al. Serum hepatitis B surface antigen levels predict surface antigen loss in hepatitis B e antigen seroconverters. Gastroenterology . 2011 Aug. 141(2):517-25, 525.e1-2. [QxMD MEDLINE Link] .
Yi Z, Jie YW, Nan Z. The efficacy of anti-viral therapy on hepatitis B virus-associated glomerulonephritis: A systematic review and meta-analysis. Ann Hepatol . 2011 Apr-Jun. 10(2):165-73. [QxMD MEDLINE Link] .
Guillevin L, Mahr A, Cohen P, et al. Short-term corticosteroids then lamivudine and plasma exchanges to treat hepatitis B virus-related polyarteritis nodosa. Arthritis Rheum . 2004 Jun 15. 51(3):482-7. [QxMD MEDLINE Link] .
Lau GK, Piratvisuth T, Luo KX, et al. Peginterferon Alfa-2a, lamivudine, and the combination for HBeAg-positive chronic hepatitis B. N Engl J Med . 2005 Jun 30. 352(26):2682-95. [QxMD MEDLINE Link] .
Marcellin P, Lau GK, Bonino F, et al. Peginterferon alfa-2a alone, lamivudine alone, and the two in combination in patients with HBeAg-negative chronic hepatitis B. N Engl J Med . 2004 Sep 16. 351(12):1206-17. [QxMD MEDLINE Link] .
Tenney DJ, Pokornowski KA, Rose RE, et al. Entecavir maintains a high genetic barrier to HBV resistance through 6 years in naive patients [abstract]. J Hepatol . 2009. 50(Suppl 1):S10.
Wong GL, Wong VW, Chan HY, et al. Undetectable HBV DNA at month 12 of entecavir treatment predicts maintained viral suppression and HBeAg-seroconversion in chronic hepatitis B patients at 3 years. Aliment Pharmacol Ther . 2012 Jun. 35(11):1326-35. [QxMD MEDLINE Link] .
Chang TT, Gish RG, de Man R, et al. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med . 2006 Mar 9. 354(10):1001-10. [QxMD MEDLINE Link] .
Chang TT, Lai CL, Kew Yoon S, et al. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology . 2010 Feb. 51(2):422-30. [QxMD MEDLINE Link] .
Schiff ER, Lee SS, Chao YC, et al. Long-term treatment with entecavir induces reversal of advanced fibrosis or cirrhosis in patients with chronic hepatitis B. Clin Gastroenterol Hepatol . 2011 Mar. 9(3):274-6. [QxMD MEDLINE Link] .
Schnittman SM, Pierce PF. Potential role of lamivudine (3TC) in the clearance of chronic hepatitis B virus infection in a patient coinfected with human immunodeficiency virus type. Clin Infect Dis . 1996 Sep. 23(3):638-9. [QxMD MEDLINE Link] .
Dienstag JL, Schiff ER, Wright TL, et al. Lamivudine as initial treatment for chronic hepatitis B in the United States. N Engl J Med . 1999 Oct 21. 341(17):1256-63. [QxMD MEDLINE Link] .
Grellier L, Mutimer D, Ahmed M, et al. Lamivudine prophylaxis against reinfection in liver transplantation for hepatitis B cirrhosis. Lancet . 1996 Nov 2. 348(9036):1212-5. [QxMD MEDLINE Link] .
Gatanaga H, Hayashida T, Tanuma J, Oka S. Prophylactic effect of antiretroviral therapy on hepatitis B virus infection. Clin Infect Dis . 2013 Jun. 56(12):1812-9. [QxMD MEDLINE Link] .
Tipples GA, Ma MM, Fischer KP, Bain VG, Kneteman NM, Tyrrell DL. Mutation in HBV RNA-dependent DNA polymerase confers resistance to lamivudine in vivo. Hepatology . 1996 Sep. 24(3):714-7. [QxMD MEDLINE Link] .
Honkoop P, Niesters HG, de Man RA, Osterhaus AD, Schalm SW. Lamivudine resistance in immunocompetent chronic hepatitis B. Incidence and patterns. J Hepatol . 1997 Jun. 26(6):1393-5. [QxMD MEDLINE Link] .
Marcellin P, Chang TT, Lim SG, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. N Engl J Med . 2003 Feb 27. 348(9):808-16. [QxMD MEDLINE Link] .
Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B. N Engl J Med . 2005 Jun 30. 352(26):2673-81. [QxMD MEDLINE Link] .
Yang H, Westland CE, Delaney WE 4th, et al. Resistance surveillance in chronic hepatitis B patients treated with adefovir dipivoxil for up to 60 weeks. Hepatology . 2002 Aug. 36(2):464-73. [QxMD MEDLINE Link] .
Villeneuve JP, Durantel D, Durantel S, et al. Selection of a hepatitis B virus strain resistant to adefovir in a liver transplantation patient. J Hepatol . 2003 Dec. 39(6):1085-9. [QxMD MEDLINE Link] .
Angus P, Vaughan R, Xiong S, et al. Resistance to adefovir dipivoxil therapy associated with the selection of a novel mutation in the HBV polymerase. Gastroenterology . 2003 Aug. 125(2):292-7. [QxMD MEDLINE Link] .
Chang TT, Lai CL. Hepatitis B virus with primary resistance to adefovir. N Engl J Med . 2006 Jul 20. 355(3):322-3; author reply 323. [QxMD MEDLINE Link] .
Hill A, Hughes SL, Gotham D, Pozniak AL. Tenofovir alafenamide versus tenofovir disoproxil fumarate: is there a true difference in efficacy and safety?. J Virus Erad . 2018 Apr 1. 4(2):72-9. [QxMD MEDLINE Link] . [Full Text] .
Heathcote J, George J, Gordon S, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-positive chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 103) [abstract]. J Hepatol . 2008. 48(suppl 2):S32.
Marcellin P, Jacobson I, Habersetzer F, et al. Tenofovir disoproxil fumarate (TDF) for the treatment of HBeAg-negative chronic hepatitis B: week 72 TDF data and week 24 adefovir dipivoxil switch data (study 102) [abstract]. J Hepatol . 2008. 48(suppl 2):S26.
Marcellin P, Heathcote EJ, Buti M, et al. Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J Med . 2008 Dec 4. 359(23):2442-55. [QxMD MEDLINE Link] .
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 86: Viral hepatitis in pregnancy. Obstet Gynecol . 2007 Oct. 110(4):941-56. [QxMD MEDLINE Link] .
US Preventive Services Task Force. Screening for hepatitis B virus infection in pregnancy: U.S. Preventive Services Task Force reaffirmation recommendation statement. Ann Intern Med . 2009 Jun 16. 150(12):869-73, W154. [QxMD MEDLINE Link] .
[Guideline] World Health Organization. Prevention of mother-to-child transmission of hepatitis B virus: guidelines on antiviral prophylaxis in pregnancy. Geneva, Switzerland. 2020 Jul. [QxMD MEDLINE Link] . [Full Text] .
Eke AC, Brooks KM, Gebreyohannes RD, Sheffield JS, Dooley KE, Mirochnick M. Tenofovir alafenamide use in pregnant and lactating women living with HIV. Expert Opin Drug Metab Toxicol . 2020 Apr. 16(4):333-42. [QxMD MEDLINE Link] .
Lin CL, Kao JH. Hepatitis B: immunization and impact on natural history and cancer incidence. Gastroenterol Clin North Am . 2020 Jun. 49(2):201-14. [QxMD MEDLINE Link] .
Vesikari T, Finn A, van Damme P, et al, for the CONSTANT Study Group. Immunogenicity and safety of a 3-antigen hepatitis B vaccine vs a single-antigen hepatitis B vaccine: a phase 3 randomized clinical trial. JAMA Netw Open . 2021 Oct 1. 4(10):e2128652. [QxMD MEDLINE Link] . [Full Text] .
Vesikari T, Langley JM, Segall N, et al, for the PROTECT Study Group. Immunogenicity and safety of a tri-antigenic versus a mono-antigenic hepatitis B vaccine in adults (PROTECT): a randomised, double-blind, phase 3 trial. Lancet Infect Dis . 2021 Sep. 21(9):1271-81. [QxMD MEDLINE Link] .
[Guideline] Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology . 2018 Apr. 67(4):1560-99. [QxMD MEDLINE Link] . [Full Text] .
Heplisav-B (hepatitis B vaccine [recombinant], adjuvanted) [package insert]. Berkeley, CA: Dynavax Technologies, Corp. November, 2017. Available at [Full Text] .
Malarkey MA, Gruber MF. Biologics License Application (BLA) approval (BL 125428) (hepatitis B vaccine (recombinant), adjuvanted [Heplisav-B]). US Food and Drug Administration. Available at https://www.fda.gov/downloads/biologicsbloodvaccines/vaccines/approvedproducts/ucm584820.pdf . November 9, 2017; Accessed: November 13, 2017.
Weir J. Biologics License Application (BLA) (BL 125428/1) supplement approval (hepatitis B vaccine (recombinant), adjuvanted [Heplisav-B]). US Food and Drug Administration. Available at https://www.fda.gov/downloads/BiologicsBloodVaccines/Vaccines/ApprovedProducts/UCM602537.pdf . March 22, 2018; Accessed: April 20, 2018.
[Guideline] Schillie S, Harris A, Link-Gelles R, Romero J, Ward J, Nelson N. Recommendations of the Advisory Committee on Immunization Practices for use of a hepatitis B vaccine with a novel adjuvant. MMWR Morb Mortal Wkly Rep . 2018 Apr 20. 67 (15):455-8. [QxMD MEDLINE Link] . [Full Text] .
Centers for Disease Control and Prevention (CDC). Use of hepatitis B vaccination for adults with diabetes mellitus: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep . 2011 Dec 23. 60(50):1709-11. [QxMD MEDLINE Link] .
Kakisaka K, Sakai A, Yoshida Y, et al. Hepatitis B surface antibody titers at one and two years after hepatitis B virus vaccination in healthy young Japanese adults. Intern Med . 2019 Aug 15. 58(16):2349-55. [QxMD MEDLINE Link] . [Full Text] .
Juday T, Tang H, Harris M, Powers AZ, Kim E, Hanna GJ. Adherence to chronic hepatitis B treatment guideline recommendations for laboratory monitoring of patients who are not receiving antiviral treatment. J Gen Intern Med . 2011 Mar. 26(3):239-44. [QxMD MEDLINE Link] . [Full Text] .
El-Serag HB, Davila JA. Surveillance for hepatocellular carcinoma: in whom and how?. Therap Adv Gastroenterol . 2011 Jan. 4(1):5-10. [QxMD MEDLINE Link] . [Full Text] .
Hoofnagle JH. Reactivation of hepatitis B. Hepatology . 2009 May. 49(5 suppl):S156-65. [QxMD MEDLINE Link] . [Full Text] .
Hagiyama H, Kubota T, Komano Y, Kurosaki M, Watanabe M, Miyasaka N. Fulminant hepatitis in an asymptomatic chronic carrier of hepatitis B virus mutant after withdrawal of low-dose methotrexate therapy for rheumatoid arthritis. Clin Exp Rheumatol . 2004 May-Jun. 22(3):375-6. [QxMD MEDLINE Link] .
Narvaez J, Rodriguez-Moreno J, Martinez-Aguila MD, Clavaguera MT. Severe hepatitis linked to B virus infection after withdrawal of low dose methotrexate therapy. J Rheumatol . 1998 Oct. 25(10):2037-8. [QxMD MEDLINE Link] .
Markovic S, Drozina G, Vovk M, Fidler-Jenko M. Reactivation of hepatitis B but not hepatitis C in patients with malignant lymphoma and immunosuppressive therapy. A prospective study in 305 patients. Hepatogastroenterology . 1999 Sep-Oct. 46(29):2925-30. [QxMD MEDLINE Link] .
Sheen IS, Liaw YF, Lin SM, Chu CM. Severe clinical rebound upon withdrawal of corticosteroid before interferon therapy: incidence and risk factors. J Gastroenterol Hepatol . 1996 Feb. 11(2):143-7. [QxMD MEDLINE Link] .
Navarro R, Vilarrasa E, Herranz P, et al. Safety and effectiveness of ustekinumab and antitumour necrosis factor therapy in patients with psoriasis and chronic viral hepatitis B or C: a retrospective, multicentre study in a clinical setting. Br J Dermatol . 2013 Mar. 168(3):609-16. [QxMD MEDLINE Link] .
Germanidis G, Hytiroglou P, Zakalka M, Settas L. Reactivation of occult hepatitis B virus infection, following treatment of refractory rheumatoid arthritis with abatacept. J Hepatol . 2012 Jun. 56(6):1420-1. [QxMD MEDLINE Link] .
[Guideline] European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol . 2017 Aug. 67 (2):370-98. [QxMD MEDLINE Link] .
[Guideline] Abara WE, Qaseem A, Schillie S, McMahon BJ, Harris AM, for the High Value Care Task Force of the American College of Physicians and the Centers for Disease Control and Prevention. Hepatitis B vaccination, screening, and linkage to care: best practice advice from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med . 2017 Dec 5. 167 (11):794-804. [QxMD MEDLINE Link] .
Phillips D. Clinical guideline on HBV released by ACP, CDC. Medscape Medical News. Available at https://www.medscape.com/viewarticle/888975 . November 21, 2017; Accessed: January 16, 2018.
[Guideline] European Association for the Study of the Liver. EASL clinical practice guidelines for the management of patients with decompensated cirrhosis. J Hepatol . 2018 Aug. 69 (2):406-60. [QxMD MEDLINE Link] .
[Guideline] European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol . 2018 Jul. 69 (1):182-236. [QxMD MEDLINE Link] .
[Guideline] Gordan JD, Kennedy EB, Abou-Alfa GK, et al. Systemic therapy for advanced hepatocellular carcinoma: ASCO guideline. J Clin Oncol . 2020 Dec 20. 38(36):4317-45. [QxMD MEDLINE Link] . [Full Text] .
CDC. Viral hepatitis surveillance report 2018 — hepatitis B. Centers for Disease Control and Prevention. Available at https://www.cdc.gov/hepatitis/statistics/2018surveillance/HepB.htm . 2020 July 27; Accessed: Acessed: October 26, 2020.
Smith BD, Morgan RL, Beckett GA, et al. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945-1965. MMWR Recomm Rep . 2012 Aug 17. 61:1-32. [QxMD MEDLINE Link] . [Full Text] .
Chou R, Cottrell EB, Wasson N, Rahman B, Guise JM. Screening for hepatitis C virus infection in adults: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med . 2013 Jan 15. 158(2):101-8. [QxMD MEDLINE Link] .
Lai CL, Gane E, Liaw YF, et al. Telbivudine (LdT) vs. lamivudine for chronic hepatitis B: first-year results from the international phase III GLOBE trial [abstract]. Hepatology . 2005. 42:748A.
Liaw YF, Gane E, Leung N, et al. 2-Year GLOBE trial results: telbivudine Is superior to lamivudine in patients with chronic hepatitis B. Gastroenterology . 2009 Feb. 136(2):486-95. [QxMD MEDLINE Link] .
Behre U, Bleckmann G, Crasta PD, et al. Long-term anti-HBs antibody persistence and immune memory in children and adolescents who received routine childhood hepatitis B vaccination. Hum Vaccin Immunother . 2012 Jun. 8(6):813-8. [QxMD MEDLINE Link] .
[Guideline] Chustecka Z. Boxed warning on HBV reactivation for blood cancer drugs. Medscape Medical News. Available at https://www.medscape.com/viewarticle/811629 . September 25, 2013; Accessed: October 2, 2013.
[Guideline] FDA. Arzerra (ofatumumab) and Rituxan (rituximab): drug safety communication - new boxed warning, recommendations to decrease risk of hepatitis B reactivation. US Food and Drug Administration. Available at https://www.fda.gov/safety/medwatch/safetyinformation/safetyalertsforhumanmedicalproducts/ucm369846.htm . September 25, 2013; Accessed: October 2, 2013.
Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B for up to 5 years. Gastroenterology . 2006 Dec. 131(6):1743-51. [QxMD MEDLINE Link] .
Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet . 2013 Feb 9. 381(9865):468-75. [QxMD MEDLINE Link] .
Purcell RH. The discovery of the hepatitis viruses. Gastroenterology . 1993 Apr. 104(4):955-63. [QxMD MEDLINE Link] .
Tang KH, Yusoff K, Tan WS. Display of hepatitis B virus PreS1 peptide on bacteriophage T7 and its potential in gene delivery into HepG2 cells. J Virol Methods . 2009 Aug. 159(2):194-9. [QxMD MEDLINE Link] .
Thibault V, Laperche S, Akhavan S, Servant-Delmas A, Belkhiri D, Roque-Afonso AM. Impact of hepatitis B virus genotypes and surface antigen variants on the performance of HBV real time PCR quantification. J Virol Methods . 2009 Aug. 159(2):265-70. [QxMD MEDLINE Link] .
Dan C. FDA approves Vemlidy (tenofovir alafenamide) for chronic hepatitis B in adults. US Department of Health and Human Services. Available at https://www.hhs.gov/hepatitis/blog/2016/11/21/fda-approves-vemlidy-tenofovir-alafenamide-for-chronic-hepatitis-b-in-adults.html . November 21, 2016; Accessed: May 23, 2017.
US Food and Drug Administration. For patients: hepatitis B and C treatments. Available at https://www.fda.gov/forpatients/illness/hepatitisbc/ucm408658.htm . Updated: January 31, 2017; Accessed: May 23, 2017.
Gilead Sciences, Inc. US Food and Drug Administration approves Gilead’s Vemlidy (tenofovir alafenamide) for the treatment of chronic hepatitis B virus infection [press release]. Available at https://www.gilead.com/news/press-releases/2016/11/us-food-and-drug-administration-approves-gileads-vemlidy-tenofovir-alafenamide-for-the-treatment-of-chronic-hepatitis-b-virus-infection . November 10, 2017; Accessed: May 23, 2017.
Zhao Q, Liu K, Zhu X, et al. Anti-viral effect in chronic hepatitis B patients with normal or mildly elevated alanine aminotransferase. Antiviral Res . 2020 Oct 13. 184:104953. [QxMD MEDLINE Link] . [Full Text] .
Tripathi N, Mousa OY. Hepatitis B. StatPearls [Internet] . 2020 Jan. [QxMD MEDLINE Link] . [Full Text] .
Phillips S, Jagatia R, Chokshi S. Novel therapeutic strategies for chronic hepatitis B. Virulence . 2022 Dec. 13 (1):1111-32. [QxMD MEDLINE Link] . [Full Text] .
- Hepatitis B. Under higher-power magnification, ground-glass cells may be visible in chronic hepatitis B virus (HBV) infection. Ground-glass cells are present in 50% to 75% of livers with chronic HBV infection. Immunohistochemical staining is positive for hepatitis B surface antigen (HBsAg.)
- Hepatitis B. Liver biopsy with hematoxylin stain showing stage 4 fibrosis (ie, cirrhosis) in a patient with hepatitis B.
- Hepatitis B. Hepatitis B virus (HBV) is a hepadnavirus, highly resistant to extremes of temperature and humidity, that invades the hepatocytes. The viral genome is a partially double-stranded, circular DNA linked to a DNA polymerase that is surrounded by an icosahedral nucleocapsid and then by a lipid envelope. Embedded within these layers are numerous antigens that are important in disease identification and progression. Within the nucleocapsid are the hepatitis B core antigen (HBcAg) and precore hepatitis B e antigen (HBeAg), and on the envelope is the hepatitis B surface antigen (HBsAg). Transmission electron micrograph (TEM) from Graham Colm and Wikipedia, licensed under the Creative Commons Attribution 3.0 Unported license.
- Hepatitis B. Serologic course of hepatitis B virus (HBV) infection. The flat bars show the duration of seropositivity in self-limited acute HBV infection. The pointed bars show that HBV DNA and e antigen (HBeAg) can become undetectable during chronic infection. Only immunoglobulin G (IgG) antibodies to the HBV core antigen (anti-HBc) are predictably detectable after resolution of acute hepatitis or during chronic infection. Antibody to hepatitis B surface antigen (anti-HBs) is generally detectable after resolution of acute HBV infection but may disappear with time. It is only rarely found in patients with chronic infection and does not indicate that immunologic recovery will occur or that the patient has a better prognosis. ALT = alanine transaminase. (Adapted from Liaw YF, Chu CM. Hepatitis B virus infection. Lancet. 2009;373(9663):582-92.)
- Hepatitis B. Radiologic studies may be useful in all stages of hepatitis B infection. Ultrasonography, computed tomography (CT) scanning, or magnetic resonance imaging (MRI) may exclude biliary obstruction in acute infection. In chronic disease, ultrasonograms may show nonspecific increased echogenicity of the liver parenchyma. In patients with long-standing disease, CT imaging may be used to detect cirrhosis or hepatocellular carcinoma (as shown).
- Hepatitis B. Long-standing cirrhosis leads to progressive replacement of liver parenchyma with fibrotic tissue. Over time, the liver contracts and develops a lobulated contour. These changes are readily apparent on cross-sectional imaging. This contrast-enhanced computed tomography (CT) scan demonstrates extensive cirrhosis, as well as malignant hepatocellular lesions (arrow).

Contributor Information and Disclosures
Nikolaos T Pyrsopoulos, MD, PhD, MBA, FACP, AGAF, FAASLD, FRCP(Edin) Professor and Chief, Division of Gastroenterology and Hepatology, Professor of Physiology, Pharmacology, and Neuroscience, Medical Director of Liver Transplantation, Rutgers New Jersey Medical School Nikolaos T Pyrsopoulos, MD, PhD, MBA, FACP, AGAF, FAASLD, FRCP(Edin) is a member of the following medical societies: American Association for the Study of Liver Diseases , American College of Gastroenterology , American College of Physicians , American Gastroenterological Association , American Liver Foundation , American Medical Association , American Society for Gastrointestinal Endoscopy , American Society of Transplantation , International Liver Transplantation Society , Transplantation Society Disclosure: Received research grant from: GRIFOLS. BAYER, DURECT, INTERCEPT, BEIGENE, BMS.
Ranya Selim, MD Gastroenterologist/Transplant Hepatologist Ranya Selim, MD is a member of the following medical societies: American College of Gastroenterology Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College of Pharmacy; Editor-in-Chief, Medscape Drug Reference Disclosure: Received salary from Medscape for employment. for: Medscape.
BS Anand, MD Professor, Department of Internal Medicine, Division of Gastroenterology, Baylor College of Medicine BS Anand, MD is a member of the following medical societies: American Association for the Study of Liver Diseases , American College of Gastroenterology , American Gastroenterological Association , American Society for Gastrointestinal Endoscopy Disclosure: Nothing to disclose.
George Y Wu, MD, PhD Professor, Department of Medicine, Director, Hepatology Section, Herman Lopata Chair in Hepatitis Research, University of Connecticut School of Medicine
George Y Wu, MD, PhD is a member of the following medical societies: American Association for the Study of Liver Diseases , American Gastroenterological Association , American Medical Association , American Society for Clinical Investigation , and Association of American Physicians
Disclosure: Springer Consulting fee Consulting; Gilead Consulting fee Review panel membership; Gilead Honoraria Speaking and teaching; Bristol-Myers Squibb Honoraria Speaking and teaching; Springer Royalty Review panel membership
What would you like to print?
- Print this section
- Print the entire contents of
- Print the entire contents of article
- Hepatitis in Pregnancy
- Treatment Recommendations for HIV-Infected Patients With Co-infections
- Pediatric Vaccines: Global Brands and Country Availability
- Pediatric Hepatitis B
- Polyarteritis Nodosa
- Viral Hepatitis
- Fast Five Quiz: Hepatitis B Epidemiology and Prevention
- US FDA Declines Expanded Use Of Dynavax's Hepatitis B Vaccine on Insufficient Data
- Don't Forget Adult Hepatitis Vaccinations
- Combination Therapy Looks Promising for Hepatitis D

- Drug Interaction Checker
- Pill Identifier
- Calculators

- 2002964662-overviewDiseases & Conditions Diseases & Conditions Pediatric Hepatitis B

- 2001/viewarticle/993770 Hepatitis B Vaccination Rates Lag in Patients With Psoriasis
Warning: The NCBI web site requires JavaScript to function. more...

An official website of the United States government
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- Browse Titles
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.

StatPearls [Internet].
Hepatitis b.
Nishant Tripathi ; Omar Y. Mousa .
Affiliations
Last Update: July 9, 2023 .
- Continuing Education Activity
Hepatitis B infection is a serious global healthcare problem. Often transmitted via body fluids like blood, semen, and vaginal secretions, the hepatitis B virus can cause liver injury. After infection with the hepatitis B virus, the majority of adults are able to clear the infection. Patients can present with acute symptomatic disease or have an asymptomatic disease that is identified during screening for the hepatitis B virus. This article focuses on identifying who is at risk of hepatitis B, and clinical evaluation and management of patients with hepatitis B by an interdisciplinary team. It also focuses on preventive measures.
- Describe the epidemiology of hepatitis B.
- Outline the common blood tests for the diagnosis of hepatitis B infection.
- Review the complications of hepatitis B infection.
- Explain the importance of collaboration and communication amongst the interdisciplinary teams to enhance the delivery of care for patients affected by hepatitis B.
- Introduction
Hepatitis B viral infection is a serious global healthcare problem. It is a potentially life-threatening liver infection caused by the hepatitis B virus (HBV). It is often transmitted via body fluids like blood, semen, and vaginal secretions. The majority (more than 95%) of immunocompetent adults infected with HBV can clear the infection spontaneously. Patients can present with acute symptomatic disease or have an asymptomatic infection that is identified during screening for HBV. The clinical manifestations of HBV infection vary in both acute and chronic diseases. During the acute infection, patients can have subclinical or anicteric hepatitis, icteric hepatitis, or less commonly fulminant hepatitis. In chronic infection, patients can have an asymptomatic carrier state, chronic hepatitis, cirrhosis, and hepatocellular carcinoma.
Initial symptoms are nonspecific and may include anorexia, nausea, vomiting, abdominal pain, and jaundice. In cases of severe liver damage, patients can develop jaundice, hepatic encephalopathy, ascites, gastrointestinal bleeding secondary to esophageal varices, coagulopathy, or infections. Diagnosis is based on serologic blood tests in patients with suspected signs and symptoms and associated risk factors for viral hepatitis. This will be discussed in more detail below.
Transmission of hepatitis B involves the transfer of the virus from infected people to non-immune people in various ways. Major modes of transmission for hepatitis B are as follows:
1. Horizontal transmission: It involves the transmission of hepatitis B through sexual contact or mucosal surface contact. Unprotected sex and injection drug use are major modes of transmission in low to intermediate prevalence areas. [1]
2. Vertical transmission: Vertical transmission involves the maternal-to-newborn perinatal transmission of the virus. [2] It is the predominant mode of transmission in high-prevalence areas.
Sexual contact includes unprotected intercourse (vaginal, oral, or anal) and mucosal contact involves any contact involving an infected patient’s saliva, vaginal secretion, semen, and blood.
Prevalence areas are based on the percentage of the population with hepatitis B surface antigen (HBsAg) positivity with greater than or equal to 8% representing high prevalence areas, 2-7% representing low to intermediate prevalence areas, and less than 2% representing low prevalence areas. [3]
- Epidemiology
HBV infection has the potential for progression to a chronic state and thus presents as a global public health threat for its associated morbidity and mortality. While hepatitis B vaccines are available, limited access to healthcare and lack of proper health education contributes to the increasing global prevalence of hepatitis B. Lower incidence of hepatitis B in the United States compared to Asia and Africa is due to better access to healthcare and better use of vaccinations and other preventive measures.
U.S. Statistics
- Around 60,000 new cases of HBV infection annually [4]
- 2 million or more people with chronic hepatitis B infection [4]
- Prevalence is higher in black, Hispanic, and Asian populations compared to whites [5]
- Prevalence is lower in people less than 12 years of age born in the U.S.
- Accounts for 5% to 10% of chronic end-stage liver disease, and 10% to 15% of cases of hepatocellular cancer
- Causes 5000 deaths annually
Worldwide Statistics
- 350-400 million of the world population has chronic hepatitis B. [6]
- The following population is known to have a higher prevalence: Asian Pacific Islanders, Alaskan Eskimos, and Australian aborigines. [6]
- The following geographic regions have higher prevalence: the Indian sub-continent, sub-Saharan Africa, and central Asia.
- The prevalence of hepatitis B is reduced after the initiation of the hepatitis B vaccination program.
- 10 genotypes (A-J) of hepatitis B have been identified. [7]
High-risk groups for HBV infection include intravenous drug users, infants born to infected mothers, males who have sexual intercourse with other males, hemodialysis patients (and workers), healthcare workers, household contacts of known patients with chronic HBV. A majority of the global HBV disease burden is primarily through vertical transmission.
- Pathophysiology
Hepatitis B virus is transmitted via percutaneous inoculation or through mucosal exposure with infectious bodily fluids. Oral-fecal transmission is possible but considerably rare. The incubation period of HBV infection is typically between 30 and 180 days, and while recovery is common in immunocompetent patients, a small percentage can progress to a chronic state, serologically defined as the presence of HBsAg for greater than six months. HBsAg is transmitted via blood contact or body secretions, and the risk of acquiring hepatitis B is considerably higher in individuals with close contact with HBsAg-positive patients.
The pathogenesis of liver disease in HBV infection is mainly immune-mediated, and in some circumstances, HBV can cause direct cytotoxic injury to the liver. HBsAg and other nucleocapsid proteins that are present on cell membranes promote T cells-induced cellular lysis of HBV-infected cells. Cytotoxic T cell response to HBV-infected hepatocytes is relatively ineffective; a significant majority of HBV DNA is cleared from the hepatic system prior to maximal T cell infiltration, suggesting that the immune response is likely more robust in the early stages of infection. The immune response may not be the sole etiology behind hepatic injury in hepatitis B patients. Hepatitis B-associated injury is also seen in post-liver transplant patients with hepatitis B that are on immunosuppressant therapy. The histological pattern that follows from this infection is termed fibrosing cholestatic hepatitis and is thought to be associated with an overwhelming exposure to HBsAg. This lends credence to the idea that hepatitis B may possess pathogenicity regardless of the immune system’s response. [8]
- Histopathology
Acute Hepatitis B Infection: Histologic findings include "lobular disarray, ballooning degeneration, multiple apoptotic bodies, Kupffer cell activation, and lymphocyte-predominant lobular and portal inflammation. [9]
Chronic Hepatitis B Infection: Lymphocyte-predominant portal inflammation with interface hepatitis and spotty lobular inflammation. [9]
- History and Physical
Patients infected with HBV could be asymptomatic initially and, depending on the particular genotype, might not be symptomatic throughout the infected state. In these particular cases, careful history taking is important to establish a diagnosis. However, when symptomatic from acute HBV infection, patients can present with serum sickness-like syndrome manifested as fever, skin rash, arthralgia, and arthritis. This syndrome usually subsides with the onset of jaundice. Patients may also have fatigue, abdominal pain, nausea, and anorexia.
History taking should emphasize the social history, including sexual practices (e.g., unprotected, same-sex, etc.), illicit drug use, profession (e.g., healthcare worker, sex worker), and living arrangements (i.e., within the same household as a patient with HBV infection). Patients in high-risk groups (i.e., healthcare workers, IV substance abuse patients, etc.) or those from highly endemic areas may warrant testing. Those with certain mental illnesses like bipolar disorder, schizophrenia, or manic disorder are at an increased risk for contracting HBV infection during manic states within which one may participate in risky sexual behaviors, including unprotected sex.
Physical examination should also assess for stigmata of chronic liver disease, including jaundice, ascites, hepatomegaly, splenomegaly, palmar erythema, Dupuytren contractures, spider nevi, gynecomastia, caput medusa, and hepatic encephalopathy which suggests portal hypertension and cirrhosis.
Extrahepatic manifestations include polyarteritis nodosa and glomerular disease (membranous nephropathy and, less often, membranoproliferative glomerulonephritis). Aplastic anemia has also been described.
Diagnosis of Hepatitis B is based on proper history taking, physical examination, laboratory works, and imaging.
Initial symptoms are nonspecific and can include anorexia, nausea, vomiting, abdominal pain, dark urine, clay-colored stool, and jaundice. In cases of severe liver damage, advanced findings specific to liver damage are common and can include hepatic encephalopathy, confusion, coma, ascites, gastrointestinal bleeding, coagulopathy, or infections. In cases of chronic hepatitis B, patients can have a chronic inactive infection, or they can develop findings of acute hepatitis known as chronic active hepatitis.
The diagnosis of hepatitis B relies on the appropriate history/physical and evaluation of serum or viral biomarkers. Viral serology of hepatitis B is usually detectable 1-12 weeks after initial infection with the primary viral marker being hepatitis B surface antigen (HBsAg). The presence of HBsAg rarely persists beyond 6 months after infection and typically precedes detectable quantities of the corresponding antibody to surface antigen (Anti-HBsAg). The period of time between the disappearance of HBsAg and the appearance of Anti-HBsAg is termed “the window period” or “serological gap.” During the window period, other viral serology could also be undetectable. HBsAg is the first virological marker to be detected thanks to its exposure on the viral surface and is indicative of an acute infection. Immune-mediated destruction of the nucleocapsid allows exposure of core antigen (HBcAg) or e antigen (HBeAg) with subsequent antibody development. Liver enzymes are typically elevated within the latter part of the replicative phase on infection thanks to active inflammatory processes, otherwise, liver transaminases could also be within their reference ranges. Hence, liver transaminases should not be a sole guide to diagnosing suspected hepatitis B infection.
The presence of antibodies to HBsAg indicates immunized status while the presence of antibodies to HBeAg refers to a possible chronic infection state. Seroconversion refers to the transition between an acute, immune-active phase to an inactive carrier state and is marked by the spontaneous development of antibodies to HBeAg. Earlier seroconversion has been related to more favorable outcomes while later seroconversion, in conjunction with recurrent bouts of reactivation and remission, is more liable to complications like liver cirrhosis, thus resulting in poorer outcomes. [10] The persistence of serum HBsAg for a duration of 6 months or greater delineates acute hepatitis B infection from chronic hepatitis B infection. Following groups of people should be screened for hepatitis B: [3]
- Persons born in high or intermediate endemic areas (HBsAg prevalence of greater than or equal to 2%). African countries, countries from North, Southeast, and East Asia. All countries from Australia and South Pacific (except for Australia and New Zealand). All countries from the Middle East (except for Israel and Cyprus). All countries from Eastern Europe (except for Hungary), Western Europe (Spain, Malta, and the indigenous population of Greenland), North America (Alaskan natives and indigenous populations of Northern Canada), Mexico, Guatemala, and Honduras. South America (Ecuador, Guyana, Suriname, Venezuela, and Amazonian areas). Caribbean (Antigua, Barbuda, Dominica, Grenada, Haiti, Jamaica, Saint Kitts and Nevis, Saint Lucia, and Turks and Caicos Islands).
- The unvaccinated U.S. citizens whose parents were born in high prevalence areas.
- History of illicit intravenous drug use.
- Men who have sex with men.
- Persons on immunosuppressive therapy.
- Persons with elevated ALT or AST of unknown origin.
- Blood, plasma, organ, tissues, or semen donors.
- Persons with end-stage renal disease.
- All pregnant women and infants born to HBsAg-positive mothers.
- Persons with chronic liver disease and HIV.
- Close contacts of HBsAg-positive persons, such as household, sexual, or needle-sharing.
- Persons with more than one sexual partner in the last six months.
- Persons requesting evaluation or treatment for sexually transmitted infections.
- Health care workers or public safety workers who are at risk for occupational exposure to blood or blood-contaminated body fluids.
- Residents and staff at facilities for developmentally disabled persons.
- Travelers to countries with an intermediate or high prevalence of Hepatitis B virus infection.
- Correctional facilities inmates.
- 19-59-year-old persons with diabetes who have not been vaccinated for Hepatitis B.
- Persons who are the source of blood or body fluid exposures that might require post-exposure prophylaxis.
Interpretation of Serologic Markers
Following serologic markers are often tested: Hepatitis B surface antigen (HBsAg), antibody to Hepatitis B surface antigen (anti-HBs), Hepatitis B core Ab (Anti-HBc) IgM, Hepatitis B core Ab (Anti-HBc) IgG, Hepatitis B e antigen (HBeAg), and Hepatitis B e antibody (anti-HBe). [10]
HBsAg: Acute infection (less than 6 months) or chronic infection (more than 6 months).
Anti-HBs: Recovery from acute infection or immunity from vaccination.
HBeAg: Mostly associated with high viral load.
Anti-HBe: Low replicative phase.
Anti-HBc IgM: Acute infection, an only marker present in the window period, can be present during exacerbation of chronic infection.
Anti-HBc IgG: Exposure to infection, chronic infection (if present along with HBsAg), recovery from acute infection (if present with anti-HBs), if isolated presence, may represent occult infection.
Other markers are: Hepatitis B viral DNA is for detection of viral load. Hepatitis B genotype provides input about disease progression and response to interferons. [11]
- Treatment / Management
Preventive measures constitute a major component of the management of hepatitis B. As of 2019, hepatitis B vaccines available in the United States are categorized into either single-antigen hepatitis B vaccines or combination vaccines.
Acute hepatitis B infection is self cleared in 95% of healthy adults. Management is supportive in a majority of patients. Patients with severe acute disease (2 of the 3: bilirubin more than 10 mg/dl, INR more than 1.6 and hepatic encephalopathy) and protracted acute severe disease (total bilirubin more than 3 mg/dl or direct bilirubin more than 1.5 mg/dl, INR more than 1.5, hepatic encephalopathy, or ascites) need antiviral treatment.
Management of chronic hepatitis B should include identification of HIV, hepatitis C, and hepatitis D coinfection, hepatitis B virus replication status, and severity of the disease. [10] The severity of the disease is based on clinical assessment, blood counts, liver enzymes, and liver histology. [10] While non-invasive tests are useful (blood test, imaging to measure liver stiffness) for chronic hepatitis B with normal alanine transferase, for patients with elevated or fluctuating alanine transferase, liver biopsy is necessary to identify if they need antiviral treatment. [10]
FDA-approved medications for chronic hepatitis B include interferons (peginterferon alfa-2a, interferon alfa-2b), nucleoside analogs (entecavir, lamivudine, telbivudine), and nucleotide analogs (adefovir, tenofovir). Entecavir and tenofovir are preferred for acute HBV infection if treatment is warranted, due to their relatively higher barrier to resistance. Entecavir combination drugs have been developed. However, a 2018 meta-analysis based on 24 studies involved with entecavir polytherapy vs entecavir monotherapy determined that entecavir combination drugs were no more effective than entecavir monotherapy. [12] Vertical transmission of hepatitis B remains a significant cause of the global HBV burden. In a 2015 prospective, multicenter trial, administration of tenofovir in HBsAg-positive and/or HBeAg-positive mothers demonstrated a benefit in reducing ALT levels in mothers and decreasing infant HBsAg levels at 6 months postpartum. [13] Major drawbacks for this study, however, include a relatively small sample size (n=118) and the lack of a placebo-based control group. Oral nucleos(t)ide therapy has been shown to suppress viral replication and thus decrease the viral burden. Lamivudine was the first effective agent to successfully used to suppress viral counts but was associated with high drug resistance. [14] A 2014 clinical trial comparing entecavir vs lamivudine in chronic B hepatitis reported better virological response in the entecavir group compared to the lamivudine group. [15] The 2013 GAHB trial was a placebo-controlled, double-blind study that compared lamivudine with a placebo. HBsAg clearance was achieved in a majority of patients with lamivudine therapy but the overall strength of the study was weakened by low recruitment numbers (n = 35). [16] For patients in the immune-tolerant phase of hepatitis B infection, a stage marked by normal liver transaminases and HBV DNA, antiviral medications were not recommended. A randomized controlled study showed suboptimal control of viral burden, likely secondary to high circulating levels of HBV DNA. [17] Regarding monotherapy versus combined therapy, there have been several limited studies addressing this issue. In the 2018 POTENT study, there was no demonstrated difference between monotherapy versus sequential therapy although there was insufficient data for statistical significance for HBsAg seroconversion. [18]
The counseling of patients on the prevention of transmission is extremely valuable. Lifestyle modifications include reducing intake of agents with potential for liver damage such as alcohol, hepatotoxic medications, herbal medications, and herbal supplements.
The goals of antiviral therapy are: [10]
- Suppression of hepatitis B virus replication
- Reduction of liver inflammation
- Prevention of progression to liver cirrhosis and hepatocellular carcinoma
Appropriate treatment response is indicated by the following findings: [10]
- Blood tests: normalization of ALT
- Undetectable hepatitis B viral DNA
- Loss of HBsAg and HBeAg with seroconversion to anti-HBs and anti-HBe
- Reduced inflammation on liver biopsy with no worsening of fibrosis
Surgical intervention for hepatitis B is only indicated for fulminant liver disease requiring transplantation.
- Differential Diagnosis
The differential diagnosis for hepatitis B infection is broad due to the presence of non-specific symptoms such as fatigue, abdominal pain, nausea, and vomiting. Other etiologies of hepatitis (i.e., hepatitis A, hepatitis C, hepatitis E, alcoholic hepatitis, and autoimmune hepatitis) should be considered in conjunction with appropriate history taking and pertinent laboratory investigation.
Iron overload (hemochromatosis) can be associated with abdominal tenderness and abnormal liver transaminase levels. Pertinent findings that favor a diagnosis of hemochromatosis compared to hepatitis B include diffuse skin discoloration (bronze diabetes) and impaired glucose tolerance.
Wilson disease is a disease of excessive copper accumulation. It is associated with psychiatric disturbances due to copper accumulation in the basal ganglia. Kayser-Fleischer rings are pathognomonic for Wilson disease but are not completely sensitive (requires an expert ophthalmologist to confirm this finding). Laboratory evaluation that favors a diagnosis of Wilson disease includes low serum ceruloplasmin levels and elevated urinary copper, and if abnormal, requires further evaluation by a hepatologist.
- Alcoholic hepatitis
- Autoimmune hepatitis
- Drug-induced liver injury
- Hemochromatosis
- Hepatitis A
- Hepatitis C
- Hepatitis D
- Hepatitis E
- Hepatocellular carcinoma
- Human immunodeficiency virus
- Wilson disease
Acute HBV infection can be treated symptomatically and in immunocompetent patients, can spontaneously resolve. Those that progress to the chronic state, however, are at increased risk for the development of hepatocellular carcinoma, cirrhosis, or fulminant liver failure. The likelihood of risk is dependent on the particular genotype, and the method of transmission as vertical transmission has a higher risk of long-term complications compared to horizontal transmission cases.
- Complications
Unlike hepatitis A and hepatitis E, in which there is no chronic state, HBV infection has the potential for the development of a chronic state. Chronic hepatitis B predisposes a patient to the development of portal hypertension, cirrhosis, and its complications or hepatocellular carcinoma (HCC). As such, patients with HBV infection should be monitored closely, and a referral to a specialist is highly recommended.Fulminant liver failure from HBV infection requires an emergent liver transplant evaluation at a liver transplant center.
- Consultations
Hepatitis B management ideally involves interprofessional collaboration. Primary care, gastroenterology, hepatology, infectious disease, liver transplant, and palliative care services are among the different services involved.
- Deterrence and Patient Education
Patient education remains one of the most important components in preventative measures regarding HBV infection.
Education should be provided to expecting parents (particularly those from highly endemic regions) about the importance of vaccination and to clarify erroneous beliefs about vaccinations.Patient education should also include counseling about the avoidance of risky behaviors that predispose an individual to be infected, including promiscuous sexual activity or intravenous drug abuse. They should also be advised not to share items such as shaving razors, toothbrushes, or hair combs due to possible transmission via mucosal contact or through microtrauma to protective barriers.
- Pearls and Other Issues
Hepatitis D (a member of the delta virus family) has been long associated with HBV infections and cannot exert pathological influence without the presence of HBV infection. Two forms of infection exist; coinfection (acquired at the same time) and superinfection (hepatitis D infection in a patient with chronic hepatitis B infection). Superinfection tends to be more severe than coinfection. Due to the preexisting hepatitis B infection, anti-HBcAg IgM is undetectable in superinfection states but can be noted in coinfection.
- Enhancing Healthcare Team Outcomes
As hepatitis B infection is highly transmissible via accidental needlesticks, healthcare providers involved in taking care of a patient with HBV should exercise caution and practice proper preventative measures such as vaccination. Patient education should also include counseling about HBV transmission. The interprofessional team's role is crucial in ensuring the best patient outcomes.
The vaccination rate is low in many developing countries, and the majority of patients are undiagnosed. Educational programs and improved awareness among the general public and healthcare providers are necessary to improve the identification of the patients, reduce transmission of the disease, and reduce the complications of hepatitis B infection.
- Review Questions
- Access free multiple choice questions on this topic.
- Comment on this article.
Disclosure: Nishant Tripathi declares no relevant financial relationships with ineligible companies.
Disclosure: Omar Mousa declares no relevant financial relationships with ineligible companies.
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.
- Cite this Page Tripathi N, Mousa OY. Hepatitis B. [Updated 2023 Jul 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
In this Page
Bulk download.
- Bulk download StatPearls data from FTP
Related information
- PMC PubMed Central citations
- PubMed Links to PubMed
Similar articles in PubMed
- China's efforts to shed its title of "Leader in liver disease". [Drug Discov Ther. 2007] China's efforts to shed its title of "Leader in liver disease". Li X, Xu WF. Drug Discov Ther. 2007 Oct; 1(2):84-5.
- Natural history of chronic hepatitis B virus infection in adults with emphasis on the occurrence of cirrhosis and hepatocellular carcinoma. [J Gastroenterol Hepatol. 2000] Natural history of chronic hepatitis B virus infection in adults with emphasis on the occurrence of cirrhosis and hepatocellular carcinoma. Chu CM. J Gastroenterol Hepatol. 2000 May; 15 Suppl:E25-30.
- Review Pharmacological interventions for acute hepatitis B infection: an attempted network meta-analysis. [Cochrane Database Syst Rev. 2017] Review Pharmacological interventions for acute hepatitis B infection: an attempted network meta-analysis. Mantzoukis K, Rodríguez-Perálvarez M, Buzzetti E, Thorburn D, Davidson BR, Tsochatzis E, Gurusamy KS. Cochrane Database Syst Rev. 2017 Mar 21; 3(3):CD011645. Epub 2017 Mar 21.
- [What General/Family Medicine Practitioner should Know about Viral Hepatitis]. [Acta Med Croatica. 2016] [What General/Family Medicine Practitioner should Know about Viral Hepatitis]. Vučak J, Vučak E. Acta Med Croatica. 2016 Apr; 70(2):87-95.
- Review Clinical aspects of hepatitis B virus infection. [Lancet. 1993] Review Clinical aspects of hepatitis B virus infection. Wright TL, Lau JY. Lancet. 1993 Nov 27; 342(8883):1340-4.
Recent Activity
- Hepatitis B - StatPearls Hepatitis B - StatPearls
Your browsing activity is empty.
Activity recording is turned off.
Turn recording back on
Connect with NLM
National Library of Medicine 8600 Rockville Pike Bethesda, MD 20894
Web Policies FOIA HHS Vulnerability Disclosure
Help Accessibility Careers
COMMENTS
The clinical presentation of viral hepatitis can be nonspecific, so other etiologies of hepatitis and liver disorders may present with similar symptoms and signs commonly found in patients with viral hepatitis. Patients with acute and chronic active viral hepatitis infections may present with malaise, fatigue, low-grade fever, anorexia, nausea ...
The incubation period of hepatitis A virus (HAV) is 2-7 weeks (average, 28 days). Clinical symptoms then develop, often with a presentation similar to that of gastroenteritis or a viral respiratory infection. The most common signs and symptoms include fatigue, nausea, vomiting, fever, hepatomegaly, jaundice, dark urine, anorexia, and rash.
The clinical presentation of acute hepatitis depends on the underlying etiology. It can clinically manifest with various clinical signs and symptoms, ranging from asymptomatic elevated liver function tests to acute liver failure requiring liver transplantation. Hence, ascertaining the etiology of acute hepatitis is of utmost importance in its ...
Hepatitis A is caused by the hepatitis A virus (HAV). There were an estimated 4,500 acute infections in 2022. Hepatitis B. Hepatitis B is caused by the hepatitis B virus (HBV). There were an estimated 13,888 acute infections in 2022. There were an estimated 640,000 adults with chronic HBV infection during January 2017-March 2020. Hepatitis C
Hepatitis means inflammation of the liver. The liver is one of the largest and most important organs in a person's body. The liver is about the size of a football and, on average, weighs about 3 pounds. It is located on the upper right side of a person's body, behind the lower ribs. Almost all the blood in a person's body passes through the liver.
Appetite usually returns after the first week of symptoms. Acute viral hepatitis usually resolves spontaneously 4 to 8 weeks after symptom onset. Anicteric hepatitis (hepatitis without jaundice) occurs more often than icteric hepatitis in patients with HCV infection and in children with HAV infection. It typically manifests as a minor flu-like ...
Hepatitis, a general term referring to inflammation of the liver, may result from various causes, both infectious (ie, viral, bacterial, fungal, and parasitic organisms) and noninfectious (eg, alcohol, drugs, autoimmune diseases, and metabolic diseases); this article focuses on viral hepatitis, which accounts for more than 50% of cases of acute hepatitis in the United States, primarily in the ...
Hepatitis refers to an inflammatory condition of the liver. It is commonly the result of a viral infection, but there are other possible causes of hepatitis. These include autoimmune hepatitis and ...
Less commonly, hepatitis results from a reaction of the immune system that causes inflammation of the liver (autoimmune hepatitis), genetic liver disorders, and other viral infections (such as infectious mononucleosis, herpes simplex, or cytomegalovirus infection). SARS-CoV-2 infection (COVID-19) can cause hepatitis that is usually mild.
Safe and effective vaccines are available to prevent hepatitis B virus (HBV). This vaccine also prevents the development of hepatitis D virus (HDV) and given at birth strongly reduces transmission risk from mother to child. Chronic hepatitis B infection can be treated with antiviral agents.
Hepatitis is an inflammation of the liver often caused by a virus. Learn about viral hepatitis, statistics, surveillance, resources, populations and impact. View All For Everyone. Basics Outbreak Linked to Frozen Organic Strawberries Outbreak Linked to Fresh Organic Strawberries Prevention Approaches for Viral Hepatitis in Gay and Bisexual Men ...
Hepatitis is a general term used to describe inflammation of the liver. Liver inflammation can be caused by several viruses (viral hepatitis), chemicals, drugs, alcohol, certain genetic disorders or by an overactive immune system that mistakenly attacks the liver, called autoimmune hepatitis. Depending on its course, hepatitis can be acute ...
Symptoms of all types of viral hepatitis are similar and can include one or more of the following: Jaundice • Fever • Fatigue • Loss of appetite • Nausea • Vomiting • Abdominal pain • Joint pain. <30% of children <6 years of age have symptoms (which typically do not include jaundice)
History. Along with outlining the presenting complaint and its severity and sequelae, the history should also initiate a search for the source of exposure (eg, overseas travel, lack of immunization, intravenous [IV] drug use) and attempt to exclude other possible causes of acute hepatitis (eg, accidental acetaminophen overdose).
Fulminant hepatitis B is believed to be due to massive immune-mediated lysis of infected hepatocytes. This explains why many patients with fulminant hepatitis B have no evidence of HBV replication at presentation . The reasons why HBV has a fulminant course in some patients are not well-understood.
Clinical presentation varies from asymptomatic infection in two-thirds of patients to icteric hepatitis and, rarely, fulminant liver failure. A serum-sickness-like illness, characterized by fever, arthralgias, and rash, may occur in the prodromal period, followed by constitutional symptoms, anorexia, nausea, jaundice, and right upper quadrant ...
The vaccine provides long-term protection against clinical illness and chronic hepatitis B virus infection. Because of the vaccine, cases of acute hepatitis B infections have notably decreased in the United States. Contact C-ASSIST Family Health Clinic Today! Call (313) 670-9943 for more information.
Appetite usually returns after the first week of symptoms. Acute viral hepatitis usually resolves spontaneously 4 to 8 weeks after symptom onset. Anicteric hepatitis (hepatitis without jaundice) occurs more often than icteric hepatitis in patients with HCV infection and in children with HAV infection. It typically manifests as a minor flu-like ...
For health professionals, learn more about hepatitis A symptoms, how long it takes for symptoms to d. Skip directly to site content Skip directly to search. ... Disease presentation. Older children and adults with HAV infection will typically experience symptoms. Most (70%) of infections in children younger than age 6 are not accompanied by ...
Hepatitis B is a worldwide healthcare problem, especially in developing areas. An estimated one third of the global population has been infected with the hepatitis B virus (HBV). ... Presentation History. Inquire into patients' sexual history, occupational history, illicit drug use, and any contacts with known infection. ...
Hepatitis B viral infection is a serious global healthcare problem. It is a potentially life-threatening liver infection caused by the hepatitis B virus (HBV). It is often transmitted via body fluids like blood, semen, and vaginal secretions. The majority (more than 95%) of immunocompetent adults infected with HBV can clear the infection spontaneously. Patients can present with acute ...