- Cookies & Privacy
- GETTING STARTED
- Introduction
- FUNDAMENTALS
- Acknowledgements
- Research questions & hypotheses
- Concepts, constructs & variables
- Research limitations
- Getting started
- Sampling Strategy
- Research Quality
- Research Ethics
- Data Analysis

Types of quantitative research question
Dissertations that are based on a quantitative research design attempt to answer at least one quantitative research question . In some cases, these quantitative research questions will be followed by either research hypotheses or null hypotheses . However, this article focuses solely on quantitative research questions. Furthermore, since there is more than one type of quantitative research question that you can attempt to answer in a dissertation (i.e., descriptive research questions, comparative research questions and relationship-based research questions), we discuss each of these in this article. If you do not know much about quantitative research and quantitative research questions at this stage, we would recommend that you first read the article, Quantitative research questions: What do I have to think about , as well as an overview article on types of variables , which will help to familiarise you with terms such as dependent and independent variable , as well as categorical and continuous variables [see the article: Types of variables ]. The purpose of this article is to introduce you to the three different types of quantitative research question (i.e., descriptive, comparative and relationship-based research questions) so that you can understand what type(s) of quantitative research question you want to create in your dissertation. Each of these types of quantitative research question is discussed in turn:
Descriptive research questions
Comparative research questions.
- Relationship-based research questions
Descriptive research questions simply aim to describe the variables you are measuring. When we use the word describe , we mean that these research questions aim to quantify the variables you are interested in. Think of research questions that start with words such as "How much?" , "How often?" , "What percentage?" , and "What proportion?" , but also sometimes questions starting "What is?" and "What are?" . Often, descriptive research questions focus on only one variable and one group, but they can include multiple variables and groups. We provide some examples below:
| Question: | How many calories do Americans consume per day? |
| Variable: | Daily calorific intake |
| Group: | Americans |
| Question: | How many calories do American men and women consume per day? |
| Variable: | Daily calorific intake |
| Group: | 1. American men 2. American women |
| Question: | How often do British university students use Facebook each week? |
| Variable: | Weekly Facebook usage |
| Group: | British university students |
| Question: | How often do male and female British university students upload photos and comment on other users' photos on Facebook each week? |
| Variable: | 1. Weekly photo uploads on Facebook 2. Weekly comments on other users? photos on Facebook |
| Group: | 1. Male, British university students 2. Female, British university students |
| Question: | What are the most important factors that influence the career choices of Australian university students? |
| Variable: | Factors influencing career choices |
| Group: | Australian university students |
In each of these example descriptive research questions, we are quantifying the variables we are interested in. However, the units that we used to quantify these variables will differ depending on what is being measured. For example, in the questions above, we are interested in frequencies (also known as counts ), such as the number of calories, photos uploaded, or comments on other users? photos. In the case of the final question, What are the most important factors that influence the career choices of Australian university students? , we are interested in the number of times each factor (e.g., salary and benefits, career prospects, physical working conditions, etc.) was ranked on a scale of 1 to 10 (with 1 = least important and 10 = most important). We may then choose to examine this data by presenting the frequencies , as well as using a measure of central tendency and a measure of spread [see the section on Data Analysis to learn more about these and other statistical tests].
However, it is also common when using descriptive research questions to measure percentages and proportions , so we have included some example descriptive research questions below that illustrate this.
| Question: | What percentage of American men and women exceed their daily calorific allowance? |
| Variable: | Daily calorific intake |
| Group: | 1. American men 2. American women |
| Question: | What proportion of British male and female university students use the top 5 social networks? |
| Variable: | Use of top 5 social networks (i.e. Facebook, MySpace, Twitter, LinkedIn, and Classmates) |
| Group: | 1. Male, British university students 2. Female, British university students |
In terms of the first descriptive research question about daily calorific intake , we are not necessarily interested in frequencies , or using a measure of central tendency or measure of spread , but instead want understand what percentage of American men and women exceed their daily calorific allowance . In this respect, this descriptive research question differs from the earlier question that asked: How many calories do American men and women consume per day? Whilst this question simply wants to measure the total number of calories (i.e., the How many calories part that starts the question); in this case, the question aims to measure excess ; that is, what percentage of these two groups (i.e., American men and American women) exceed their daily calorific allowance, which is different for males (around 2500 calories per day) and females (around 2000 calories per day).
If you are performing a piece of descriptive , quantitative research for your dissertation, you are likely to need to set quite a number of descriptive research questions . However, if you are using an experimental or quasi-experimental research design , or a more involved relationship-based research design , you are more likely to use just one or two descriptive research questions as a means to providing background to the topic you are studying, helping to give additional context for comparative research questions and/or relationship-based research questions that follow.
Comparative research questions aim to examine the differences between two or more groups on one or more dependent variables (although often just a single dependent variable). Such questions typically start by asking "What is the difference in?" a particular dependent variable (e.g., daily calorific intake) between two or more groups (e.g., American men and American women). Examples of comparative research questions include:
| Question: | What is the difference in the daily calorific intake of American men and women? |
| Dependent variable: | Daily calorific intake |
| Groups: | 1. American men 2. American women |
| Question: | What is the difference in the weekly photo uploads on Facebook between British male and female university students? |
| Dependent variable: | Weekly photo uploads on Facebook |
| Groups: | 1. Male, British university students 2. Female, British university students |
| Question: | What are the differences in usage behaviour on Facebook between British male and female university students? |
| Dependent variable: | Usage behaviour on Facebook (e.g. logins, weekly photo uploads, status changes, commenting on other users' photos, app usage, etc.) |
| Group: | 1. Male, British university students 2. Female, British university students |
| Question: | What are the differences in perceptions towards Internet banking security between adolescents and pensioners? |
| Dependent variable: | Perceptions towards Internet banking security |
| Groups: | 1. Adolescents 2. Pensioners |
| Question: | What are the differences in attitudes towards music piracy when pirated music is freely distributed or purchased? |
| Dependent variable: | Attitudes towards music piracy |
| Groups: | 1. Freely distributed pirated music 2. Purchased pirated music |
Groups reflect different categories of the independent variable you are measuring (e.g., American men and women = "gender"; Australian undergraduate and graduate students = "educational level"; pirated music that is freely distributed and pirated music that is purchased = "method of illegal music acquisition").
Comparative research questions also differ in terms of their relative complexity , by which we are referring to how many items/measures make up the dependent variable or how many dependent variables are investigated. Indeed, the examples highlight the difference between very simple comparative research questions where the dependent variable involves just a single measure/item (e.g., daily calorific intake) and potentially more complex questions where the dependent variable is made up of multiple items (e.g., Facebook usage behaviour including a wide range of items, such as logins, weekly photo uploads, status changes, etc.); or where each of these items should be written out as dependent variables.
Overall, whilst the dependent variable(s) highlight what you are interested in studying (e.g., attitudes towards music piracy, perceptions towards Internet banking security), comparative research questions are particularly appropriate if your dissertation aims to examine the differences between two or more groups (e.g., men and women, adolescents and pensioners, managers and non-managers, etc.).
Relationship research questions
Whilst we refer to this type of quantitative research question as a relationship-based research question, the word relationship should be treated simply as a useful way of describing the fact that these types of quantitative research question are interested in the causal relationships , associations , trends and/or interactions amongst two or more variables on one or more groups. We have to be careful when using the word relationship because in statistics, it refers to a particular type of research design, namely experimental research designs where it is possible to measure the cause and effect between two or more variables; that is, it is possible to say that variable A (e.g., study time) was responsible for an increase in variable B (e.g., exam scores). However, at the undergraduate and even master's level, dissertations rarely involve experimental research designs , but rather quasi-experimental and relationship-based research designs [see the section on Quantitative research designs ]. This means that you cannot often find causal relationships between variables, but only associations or trends .
However, when we write a relationship-based research question , we do not have to make this distinction between causal relationships, associations, trends and interactions (i.e., it is just something that you should keep in the back of your mind). Instead, we typically start a relationship-based quantitative research question, "What is the relationship?" , usually followed by the words, "between or amongst" , then list the independent variables (e.g., gender) and dependent variables (e.g., attitudes towards music piracy), "amongst or between" the group(s) you are focusing on. Examples of relationship-based research questions are:
| Question: | What is the relationship between gender and attitudes towards music piracy amongst adolescents? |
| Dependent variable: | Attitudes towards music piracy |
| Independent variable: | Gender |
| Group: | Adolescents |
| Question: | What is the relationship between study time and exam scores amongst university students? |
| Dependent variable: | Exam scores |
| Independent variable: | Study time |
| Group: | University students |
| Question: | What is the relationship amongst career prospects, salary and benefits, and physical working conditions on job satisfaction between managers and non-managers? |
| Dependent variable: | Job satisfaction |
| Independent variable: | 1. Career prospects 2. Salary and benefits 3. Physical working conditions |
| Group: | 1. Managers 2. Non-managers |
As the examples above highlight, relationship-based research questions are appropriate to set when we are interested in the relationship, association, trend, or interaction between one or more dependent (e.g., exam scores) and independent (e.g., study time) variables, whether on one or more groups (e.g., university students).
The quantitative research design that we select subsequently determines whether we look for relationships , associations , trends or interactions . To learn how to structure (i.e., write out) each of these three types of quantitative research question (i.e., descriptive, comparative, relationship-based research questions), see the article: How to structure quantitative research questions .

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Korean Med Sci
- v.37(16); 2022 Apr 25
A Practical Guide to Writing Quantitative and Qualitative Research Questions and Hypotheses in Scholarly Articles
Edward barroga.
1 Department of General Education, Graduate School of Nursing Science, St. Luke’s International University, Tokyo, Japan.
Glafera Janet Matanguihan
2 Department of Biological Sciences, Messiah University, Mechanicsburg, PA, USA.
The development of research questions and the subsequent hypotheses are prerequisites to defining the main research purpose and specific objectives of a study. Consequently, these objectives determine the study design and research outcome. The development of research questions is a process based on knowledge of current trends, cutting-edge studies, and technological advances in the research field. Excellent research questions are focused and require a comprehensive literature search and in-depth understanding of the problem being investigated. Initially, research questions may be written as descriptive questions which could be developed into inferential questions. These questions must be specific and concise to provide a clear foundation for developing hypotheses. Hypotheses are more formal predictions about the research outcomes. These specify the possible results that may or may not be expected regarding the relationship between groups. Thus, research questions and hypotheses clarify the main purpose and specific objectives of the study, which in turn dictate the design of the study, its direction, and outcome. Studies developed from good research questions and hypotheses will have trustworthy outcomes with wide-ranging social and health implications.
INTRODUCTION
Scientific research is usually initiated by posing evidenced-based research questions which are then explicitly restated as hypotheses. 1 , 2 The hypotheses provide directions to guide the study, solutions, explanations, and expected results. 3 , 4 Both research questions and hypotheses are essentially formulated based on conventional theories and real-world processes, which allow the inception of novel studies and the ethical testing of ideas. 5 , 6
It is crucial to have knowledge of both quantitative and qualitative research 2 as both types of research involve writing research questions and hypotheses. 7 However, these crucial elements of research are sometimes overlooked; if not overlooked, then framed without the forethought and meticulous attention it needs. Planning and careful consideration are needed when developing quantitative or qualitative research, particularly when conceptualizing research questions and hypotheses. 4
There is a continuing need to support researchers in the creation of innovative research questions and hypotheses, as well as for journal articles that carefully review these elements. 1 When research questions and hypotheses are not carefully thought of, unethical studies and poor outcomes usually ensue. Carefully formulated research questions and hypotheses define well-founded objectives, which in turn determine the appropriate design, course, and outcome of the study. This article then aims to discuss in detail the various aspects of crafting research questions and hypotheses, with the goal of guiding researchers as they develop their own. Examples from the authors and peer-reviewed scientific articles in the healthcare field are provided to illustrate key points.
DEFINITIONS AND RELATIONSHIP OF RESEARCH QUESTIONS AND HYPOTHESES
A research question is what a study aims to answer after data analysis and interpretation. The answer is written in length in the discussion section of the paper. Thus, the research question gives a preview of the different parts and variables of the study meant to address the problem posed in the research question. 1 An excellent research question clarifies the research writing while facilitating understanding of the research topic, objective, scope, and limitations of the study. 5
On the other hand, a research hypothesis is an educated statement of an expected outcome. This statement is based on background research and current knowledge. 8 , 9 The research hypothesis makes a specific prediction about a new phenomenon 10 or a formal statement on the expected relationship between an independent variable and a dependent variable. 3 , 11 It provides a tentative answer to the research question to be tested or explored. 4
Hypotheses employ reasoning to predict a theory-based outcome. 10 These can also be developed from theories by focusing on components of theories that have not yet been observed. 10 The validity of hypotheses is often based on the testability of the prediction made in a reproducible experiment. 8
Conversely, hypotheses can also be rephrased as research questions. Several hypotheses based on existing theories and knowledge may be needed to answer a research question. Developing ethical research questions and hypotheses creates a research design that has logical relationships among variables. These relationships serve as a solid foundation for the conduct of the study. 4 , 11 Haphazardly constructed research questions can result in poorly formulated hypotheses and improper study designs, leading to unreliable results. Thus, the formulations of relevant research questions and verifiable hypotheses are crucial when beginning research. 12
CHARACTERISTICS OF GOOD RESEARCH QUESTIONS AND HYPOTHESES
Excellent research questions are specific and focused. These integrate collective data and observations to confirm or refute the subsequent hypotheses. Well-constructed hypotheses are based on previous reports and verify the research context. These are realistic, in-depth, sufficiently complex, and reproducible. More importantly, these hypotheses can be addressed and tested. 13
There are several characteristics of well-developed hypotheses. Good hypotheses are 1) empirically testable 7 , 10 , 11 , 13 ; 2) backed by preliminary evidence 9 ; 3) testable by ethical research 7 , 9 ; 4) based on original ideas 9 ; 5) have evidenced-based logical reasoning 10 ; and 6) can be predicted. 11 Good hypotheses can infer ethical and positive implications, indicating the presence of a relationship or effect relevant to the research theme. 7 , 11 These are initially developed from a general theory and branch into specific hypotheses by deductive reasoning. In the absence of a theory to base the hypotheses, inductive reasoning based on specific observations or findings form more general hypotheses. 10
TYPES OF RESEARCH QUESTIONS AND HYPOTHESES
Research questions and hypotheses are developed according to the type of research, which can be broadly classified into quantitative and qualitative research. We provide a summary of the types of research questions and hypotheses under quantitative and qualitative research categories in Table 1 .
| Quantitative research questions | Quantitative research hypotheses |
|---|---|
| Descriptive research questions | Simple hypothesis |
| Comparative research questions | Complex hypothesis |
| Relationship research questions | Directional hypothesis |
| Non-directional hypothesis | |
| Associative hypothesis | |
| Causal hypothesis | |
| Null hypothesis | |
| Alternative hypothesis | |
| Working hypothesis | |
| Statistical hypothesis | |
| Logical hypothesis | |
| Hypothesis-testing | |
| Qualitative research questions | Qualitative research hypotheses |
| Contextual research questions | Hypothesis-generating |
| Descriptive research questions | |
| Evaluation research questions | |
| Explanatory research questions | |
| Exploratory research questions | |
| Generative research questions | |
| Ideological research questions | |
| Ethnographic research questions | |
| Phenomenological research questions | |
| Grounded theory questions | |
| Qualitative case study questions |
Research questions in quantitative research
In quantitative research, research questions inquire about the relationships among variables being investigated and are usually framed at the start of the study. These are precise and typically linked to the subject population, dependent and independent variables, and research design. 1 Research questions may also attempt to describe the behavior of a population in relation to one or more variables, or describe the characteristics of variables to be measured ( descriptive research questions ). 1 , 5 , 14 These questions may also aim to discover differences between groups within the context of an outcome variable ( comparative research questions ), 1 , 5 , 14 or elucidate trends and interactions among variables ( relationship research questions ). 1 , 5 We provide examples of descriptive, comparative, and relationship research questions in quantitative research in Table 2 .
| Quantitative research questions | |
|---|---|
| Descriptive research question | |
| - Measures responses of subjects to variables | |
| - Presents variables to measure, analyze, or assess | |
| What is the proportion of resident doctors in the hospital who have mastered ultrasonography (response of subjects to a variable) as a diagnostic technique in their clinical training? | |
| Comparative research question | |
| - Clarifies difference between one group with outcome variable and another group without outcome variable | |
| Is there a difference in the reduction of lung metastasis in osteosarcoma patients who received the vitamin D adjunctive therapy (group with outcome variable) compared with osteosarcoma patients who did not receive the vitamin D adjunctive therapy (group without outcome variable)? | |
| - Compares the effects of variables | |
| How does the vitamin D analogue 22-Oxacalcitriol (variable 1) mimic the antiproliferative activity of 1,25-Dihydroxyvitamin D (variable 2) in osteosarcoma cells? | |
| Relationship research question | |
| - Defines trends, association, relationships, or interactions between dependent variable and independent variable | |
| Is there a relationship between the number of medical student suicide (dependent variable) and the level of medical student stress (independent variable) in Japan during the first wave of the COVID-19 pandemic? | |
Hypotheses in quantitative research
In quantitative research, hypotheses predict the expected relationships among variables. 15 Relationships among variables that can be predicted include 1) between a single dependent variable and a single independent variable ( simple hypothesis ) or 2) between two or more independent and dependent variables ( complex hypothesis ). 4 , 11 Hypotheses may also specify the expected direction to be followed and imply an intellectual commitment to a particular outcome ( directional hypothesis ) 4 . On the other hand, hypotheses may not predict the exact direction and are used in the absence of a theory, or when findings contradict previous studies ( non-directional hypothesis ). 4 In addition, hypotheses can 1) define interdependency between variables ( associative hypothesis ), 4 2) propose an effect on the dependent variable from manipulation of the independent variable ( causal hypothesis ), 4 3) state a negative relationship between two variables ( null hypothesis ), 4 , 11 , 15 4) replace the working hypothesis if rejected ( alternative hypothesis ), 15 explain the relationship of phenomena to possibly generate a theory ( working hypothesis ), 11 5) involve quantifiable variables that can be tested statistically ( statistical hypothesis ), 11 6) or express a relationship whose interlinks can be verified logically ( logical hypothesis ). 11 We provide examples of simple, complex, directional, non-directional, associative, causal, null, alternative, working, statistical, and logical hypotheses in quantitative research, as well as the definition of quantitative hypothesis-testing research in Table 3 .
| Quantitative research hypotheses | |
|---|---|
| Simple hypothesis | |
| - Predicts relationship between single dependent variable and single independent variable | |
| If the dose of the new medication (single independent variable) is high, blood pressure (single dependent variable) is lowered. | |
| Complex hypothesis | |
| - Foretells relationship between two or more independent and dependent variables | |
| The higher the use of anticancer drugs, radiation therapy, and adjunctive agents (3 independent variables), the higher would be the survival rate (1 dependent variable). | |
| Directional hypothesis | |
| - Identifies study direction based on theory towards particular outcome to clarify relationship between variables | |
| Privately funded research projects will have a larger international scope (study direction) than publicly funded research projects. | |
| Non-directional hypothesis | |
| - Nature of relationship between two variables or exact study direction is not identified | |
| - Does not involve a theory | |
| Women and men are different in terms of helpfulness. (Exact study direction is not identified) | |
| Associative hypothesis | |
| - Describes variable interdependency | |
| - Change in one variable causes change in another variable | |
| A larger number of people vaccinated against COVID-19 in the region (change in independent variable) will reduce the region’s incidence of COVID-19 infection (change in dependent variable). | |
| Causal hypothesis | |
| - An effect on dependent variable is predicted from manipulation of independent variable | |
| A change into a high-fiber diet (independent variable) will reduce the blood sugar level (dependent variable) of the patient. | |
| Null hypothesis | |
| - A negative statement indicating no relationship or difference between 2 variables | |
| There is no significant difference in the severity of pulmonary metastases between the new drug (variable 1) and the current drug (variable 2). | |
| Alternative hypothesis | |
| - Following a null hypothesis, an alternative hypothesis predicts a relationship between 2 study variables | |
| The new drug (variable 1) is better on average in reducing the level of pain from pulmonary metastasis than the current drug (variable 2). | |
| Working hypothesis | |
| - A hypothesis that is initially accepted for further research to produce a feasible theory | |
| Dairy cows fed with concentrates of different formulations will produce different amounts of milk. | |
| Statistical hypothesis | |
| - Assumption about the value of population parameter or relationship among several population characteristics | |
| - Validity tested by a statistical experiment or analysis | |
| The mean recovery rate from COVID-19 infection (value of population parameter) is not significantly different between population 1 and population 2. | |
| There is a positive correlation between the level of stress at the workplace and the number of suicides (population characteristics) among working people in Japan. | |
| Logical hypothesis | |
| - Offers or proposes an explanation with limited or no extensive evidence | |
| If healthcare workers provide more educational programs about contraception methods, the number of adolescent pregnancies will be less. | |
| Hypothesis-testing (Quantitative hypothesis-testing research) | |
| - Quantitative research uses deductive reasoning. | |
| - This involves the formation of a hypothesis, collection of data in the investigation of the problem, analysis and use of the data from the investigation, and drawing of conclusions to validate or nullify the hypotheses. | |
Research questions in qualitative research
Unlike research questions in quantitative research, research questions in qualitative research are usually continuously reviewed and reformulated. The central question and associated subquestions are stated more than the hypotheses. 15 The central question broadly explores a complex set of factors surrounding the central phenomenon, aiming to present the varied perspectives of participants. 15
There are varied goals for which qualitative research questions are developed. These questions can function in several ways, such as to 1) identify and describe existing conditions ( contextual research question s); 2) describe a phenomenon ( descriptive research questions ); 3) assess the effectiveness of existing methods, protocols, theories, or procedures ( evaluation research questions ); 4) examine a phenomenon or analyze the reasons or relationships between subjects or phenomena ( explanatory research questions ); or 5) focus on unknown aspects of a particular topic ( exploratory research questions ). 5 In addition, some qualitative research questions provide new ideas for the development of theories and actions ( generative research questions ) or advance specific ideologies of a position ( ideological research questions ). 1 Other qualitative research questions may build on a body of existing literature and become working guidelines ( ethnographic research questions ). Research questions may also be broadly stated without specific reference to the existing literature or a typology of questions ( phenomenological research questions ), may be directed towards generating a theory of some process ( grounded theory questions ), or may address a description of the case and the emerging themes ( qualitative case study questions ). 15 We provide examples of contextual, descriptive, evaluation, explanatory, exploratory, generative, ideological, ethnographic, phenomenological, grounded theory, and qualitative case study research questions in qualitative research in Table 4 , and the definition of qualitative hypothesis-generating research in Table 5 .
| Qualitative research questions | |
|---|---|
| Contextual research question | |
| - Ask the nature of what already exists | |
| - Individuals or groups function to further clarify and understand the natural context of real-world problems | |
| What are the experiences of nurses working night shifts in healthcare during the COVID-19 pandemic? (natural context of real-world problems) | |
| Descriptive research question | |
| - Aims to describe a phenomenon | |
| What are the different forms of disrespect and abuse (phenomenon) experienced by Tanzanian women when giving birth in healthcare facilities? | |
| Evaluation research question | |
| - Examines the effectiveness of existing practice or accepted frameworks | |
| How effective are decision aids (effectiveness of existing practice) in helping decide whether to give birth at home or in a healthcare facility? | |
| Explanatory research question | |
| - Clarifies a previously studied phenomenon and explains why it occurs | |
| Why is there an increase in teenage pregnancy (phenomenon) in Tanzania? | |
| Exploratory research question | |
| - Explores areas that have not been fully investigated to have a deeper understanding of the research problem | |
| What factors affect the mental health of medical students (areas that have not yet been fully investigated) during the COVID-19 pandemic? | |
| Generative research question | |
| - Develops an in-depth understanding of people’s behavior by asking ‘how would’ or ‘what if’ to identify problems and find solutions | |
| How would the extensive research experience of the behavior of new staff impact the success of the novel drug initiative? | |
| Ideological research question | |
| - Aims to advance specific ideas or ideologies of a position | |
| Are Japanese nurses who volunteer in remote African hospitals able to promote humanized care of patients (specific ideas or ideologies) in the areas of safe patient environment, respect of patient privacy, and provision of accurate information related to health and care? | |
| Ethnographic research question | |
| - Clarifies peoples’ nature, activities, their interactions, and the outcomes of their actions in specific settings | |
| What are the demographic characteristics, rehabilitative treatments, community interactions, and disease outcomes (nature, activities, their interactions, and the outcomes) of people in China who are suffering from pneumoconiosis? | |
| Phenomenological research question | |
| - Knows more about the phenomena that have impacted an individual | |
| What are the lived experiences of parents who have been living with and caring for children with a diagnosis of autism? (phenomena that have impacted an individual) | |
| Grounded theory question | |
| - Focuses on social processes asking about what happens and how people interact, or uncovering social relationships and behaviors of groups | |
| What are the problems that pregnant adolescents face in terms of social and cultural norms (social processes), and how can these be addressed? | |
| Qualitative case study question | |
| - Assesses a phenomenon using different sources of data to answer “why” and “how” questions | |
| - Considers how the phenomenon is influenced by its contextual situation. | |
| How does quitting work and assuming the role of a full-time mother (phenomenon assessed) change the lives of women in Japan? | |
| Qualitative research hypotheses | |
|---|---|
| Hypothesis-generating (Qualitative hypothesis-generating research) | |
| - Qualitative research uses inductive reasoning. | |
| - This involves data collection from study participants or the literature regarding a phenomenon of interest, using the collected data to develop a formal hypothesis, and using the formal hypothesis as a framework for testing the hypothesis. | |
| - Qualitative exploratory studies explore areas deeper, clarifying subjective experience and allowing formulation of a formal hypothesis potentially testable in a future quantitative approach. | |
Qualitative studies usually pose at least one central research question and several subquestions starting with How or What . These research questions use exploratory verbs such as explore or describe . These also focus on one central phenomenon of interest, and may mention the participants and research site. 15
Hypotheses in qualitative research
Hypotheses in qualitative research are stated in the form of a clear statement concerning the problem to be investigated. Unlike in quantitative research where hypotheses are usually developed to be tested, qualitative research can lead to both hypothesis-testing and hypothesis-generating outcomes. 2 When studies require both quantitative and qualitative research questions, this suggests an integrative process between both research methods wherein a single mixed-methods research question can be developed. 1
FRAMEWORKS FOR DEVELOPING RESEARCH QUESTIONS AND HYPOTHESES
Research questions followed by hypotheses should be developed before the start of the study. 1 , 12 , 14 It is crucial to develop feasible research questions on a topic that is interesting to both the researcher and the scientific community. This can be achieved by a meticulous review of previous and current studies to establish a novel topic. Specific areas are subsequently focused on to generate ethical research questions. The relevance of the research questions is evaluated in terms of clarity of the resulting data, specificity of the methodology, objectivity of the outcome, depth of the research, and impact of the study. 1 , 5 These aspects constitute the FINER criteria (i.e., Feasible, Interesting, Novel, Ethical, and Relevant). 1 Clarity and effectiveness are achieved if research questions meet the FINER criteria. In addition to the FINER criteria, Ratan et al. described focus, complexity, novelty, feasibility, and measurability for evaluating the effectiveness of research questions. 14
The PICOT and PEO frameworks are also used when developing research questions. 1 The following elements are addressed in these frameworks, PICOT: P-population/patients/problem, I-intervention or indicator being studied, C-comparison group, O-outcome of interest, and T-timeframe of the study; PEO: P-population being studied, E-exposure to preexisting conditions, and O-outcome of interest. 1 Research questions are also considered good if these meet the “FINERMAPS” framework: Feasible, Interesting, Novel, Ethical, Relevant, Manageable, Appropriate, Potential value/publishable, and Systematic. 14
As we indicated earlier, research questions and hypotheses that are not carefully formulated result in unethical studies or poor outcomes. To illustrate this, we provide some examples of ambiguous research question and hypotheses that result in unclear and weak research objectives in quantitative research ( Table 6 ) 16 and qualitative research ( Table 7 ) 17 , and how to transform these ambiguous research question(s) and hypothesis(es) into clear and good statements.
| Variables | Unclear and weak statement (Statement 1) | Clear and good statement (Statement 2) | Points to avoid |
|---|---|---|---|
| Research question | Which is more effective between smoke moxibustion and smokeless moxibustion? | “Moreover, regarding smoke moxibustion versus smokeless moxibustion, it remains unclear which is more effective, safe, and acceptable to pregnant women, and whether there is any difference in the amount of heat generated.” | 1) Vague and unfocused questions |
| 2) Closed questions simply answerable by yes or no | |||
| 3) Questions requiring a simple choice | |||
| Hypothesis | The smoke moxibustion group will have higher cephalic presentation. | “Hypothesis 1. The smoke moxibustion stick group (SM group) and smokeless moxibustion stick group (-SLM group) will have higher rates of cephalic presentation after treatment than the control group. | 1) Unverifiable hypotheses |
| Hypothesis 2. The SM group and SLM group will have higher rates of cephalic presentation at birth than the control group. | 2) Incompletely stated groups of comparison | ||
| Hypothesis 3. There will be no significant differences in the well-being of the mother and child among the three groups in terms of the following outcomes: premature birth, premature rupture of membranes (PROM) at < 37 weeks, Apgar score < 7 at 5 min, umbilical cord blood pH < 7.1, admission to neonatal intensive care unit (NICU), and intrauterine fetal death.” | 3) Insufficiently described variables or outcomes | ||
| Research objective | To determine which is more effective between smoke moxibustion and smokeless moxibustion. | “The specific aims of this pilot study were (a) to compare the effects of smoke moxibustion and smokeless moxibustion treatments with the control group as a possible supplement to ECV for converting breech presentation to cephalic presentation and increasing adherence to the newly obtained cephalic position, and (b) to assess the effects of these treatments on the well-being of the mother and child.” | 1) Poor understanding of the research question and hypotheses |
| 2) Insufficient description of population, variables, or study outcomes |
a These statements were composed for comparison and illustrative purposes only.
b These statements are direct quotes from Higashihara and Horiuchi. 16
| Variables | Unclear and weak statement (Statement 1) | Clear and good statement (Statement 2) | Points to avoid |
|---|---|---|---|
| Research question | Does disrespect and abuse (D&A) occur in childbirth in Tanzania? | How does disrespect and abuse (D&A) occur and what are the types of physical and psychological abuses observed in midwives’ actual care during facility-based childbirth in urban Tanzania? | 1) Ambiguous or oversimplistic questions |
| 2) Questions unverifiable by data collection and analysis | |||
| Hypothesis | Disrespect and abuse (D&A) occur in childbirth in Tanzania. | Hypothesis 1: Several types of physical and psychological abuse by midwives in actual care occur during facility-based childbirth in urban Tanzania. | 1) Statements simply expressing facts |
| Hypothesis 2: Weak nursing and midwifery management contribute to the D&A of women during facility-based childbirth in urban Tanzania. | 2) Insufficiently described concepts or variables | ||
| Research objective | To describe disrespect and abuse (D&A) in childbirth in Tanzania. | “This study aimed to describe from actual observations the respectful and disrespectful care received by women from midwives during their labor period in two hospitals in urban Tanzania.” | 1) Statements unrelated to the research question and hypotheses |
| 2) Unattainable or unexplorable objectives |
a This statement is a direct quote from Shimoda et al. 17
The other statements were composed for comparison and illustrative purposes only.
CONSTRUCTING RESEARCH QUESTIONS AND HYPOTHESES
To construct effective research questions and hypotheses, it is very important to 1) clarify the background and 2) identify the research problem at the outset of the research, within a specific timeframe. 9 Then, 3) review or conduct preliminary research to collect all available knowledge about the possible research questions by studying theories and previous studies. 18 Afterwards, 4) construct research questions to investigate the research problem. Identify variables to be accessed from the research questions 4 and make operational definitions of constructs from the research problem and questions. Thereafter, 5) construct specific deductive or inductive predictions in the form of hypotheses. 4 Finally, 6) state the study aims . This general flow for constructing effective research questions and hypotheses prior to conducting research is shown in Fig. 1 .

Research questions are used more frequently in qualitative research than objectives or hypotheses. 3 These questions seek to discover, understand, explore or describe experiences by asking “What” or “How.” The questions are open-ended to elicit a description rather than to relate variables or compare groups. The questions are continually reviewed, reformulated, and changed during the qualitative study. 3 Research questions are also used more frequently in survey projects than hypotheses in experiments in quantitative research to compare variables and their relationships.
Hypotheses are constructed based on the variables identified and as an if-then statement, following the template, ‘If a specific action is taken, then a certain outcome is expected.’ At this stage, some ideas regarding expectations from the research to be conducted must be drawn. 18 Then, the variables to be manipulated (independent) and influenced (dependent) are defined. 4 Thereafter, the hypothesis is stated and refined, and reproducible data tailored to the hypothesis are identified, collected, and analyzed. 4 The hypotheses must be testable and specific, 18 and should describe the variables and their relationships, the specific group being studied, and the predicted research outcome. 18 Hypotheses construction involves a testable proposition to be deduced from theory, and independent and dependent variables to be separated and measured separately. 3 Therefore, good hypotheses must be based on good research questions constructed at the start of a study or trial. 12
In summary, research questions are constructed after establishing the background of the study. Hypotheses are then developed based on the research questions. Thus, it is crucial to have excellent research questions to generate superior hypotheses. In turn, these would determine the research objectives and the design of the study, and ultimately, the outcome of the research. 12 Algorithms for building research questions and hypotheses are shown in Fig. 2 for quantitative research and in Fig. 3 for qualitative research.

EXAMPLES OF RESEARCH QUESTIONS FROM PUBLISHED ARTICLES
- EXAMPLE 1. Descriptive research question (quantitative research)
- - Presents research variables to be assessed (distinct phenotypes and subphenotypes)
- “BACKGROUND: Since COVID-19 was identified, its clinical and biological heterogeneity has been recognized. Identifying COVID-19 phenotypes might help guide basic, clinical, and translational research efforts.
- RESEARCH QUESTION: Does the clinical spectrum of patients with COVID-19 contain distinct phenotypes and subphenotypes? ” 19
- EXAMPLE 2. Relationship research question (quantitative research)
- - Shows interactions between dependent variable (static postural control) and independent variable (peripheral visual field loss)
- “Background: Integration of visual, vestibular, and proprioceptive sensations contributes to postural control. People with peripheral visual field loss have serious postural instability. However, the directional specificity of postural stability and sensory reweighting caused by gradual peripheral visual field loss remain unclear.
- Research question: What are the effects of peripheral visual field loss on static postural control ?” 20
- EXAMPLE 3. Comparative research question (quantitative research)
- - Clarifies the difference among groups with an outcome variable (patients enrolled in COMPERA with moderate PH or severe PH in COPD) and another group without the outcome variable (patients with idiopathic pulmonary arterial hypertension (IPAH))
- “BACKGROUND: Pulmonary hypertension (PH) in COPD is a poorly investigated clinical condition.
- RESEARCH QUESTION: Which factors determine the outcome of PH in COPD?
- STUDY DESIGN AND METHODS: We analyzed the characteristics and outcome of patients enrolled in the Comparative, Prospective Registry of Newly Initiated Therapies for Pulmonary Hypertension (COMPERA) with moderate or severe PH in COPD as defined during the 6th PH World Symposium who received medical therapy for PH and compared them with patients with idiopathic pulmonary arterial hypertension (IPAH) .” 21
- EXAMPLE 4. Exploratory research question (qualitative research)
- - Explores areas that have not been fully investigated (perspectives of families and children who receive care in clinic-based child obesity treatment) to have a deeper understanding of the research problem
- “Problem: Interventions for children with obesity lead to only modest improvements in BMI and long-term outcomes, and data are limited on the perspectives of families of children with obesity in clinic-based treatment. This scoping review seeks to answer the question: What is known about the perspectives of families and children who receive care in clinic-based child obesity treatment? This review aims to explore the scope of perspectives reported by families of children with obesity who have received individualized outpatient clinic-based obesity treatment.” 22
- EXAMPLE 5. Relationship research question (quantitative research)
- - Defines interactions between dependent variable (use of ankle strategies) and independent variable (changes in muscle tone)
- “Background: To maintain an upright standing posture against external disturbances, the human body mainly employs two types of postural control strategies: “ankle strategy” and “hip strategy.” While it has been reported that the magnitude of the disturbance alters the use of postural control strategies, it has not been elucidated how the level of muscle tone, one of the crucial parameters of bodily function, determines the use of each strategy. We have previously confirmed using forward dynamics simulations of human musculoskeletal models that an increased muscle tone promotes the use of ankle strategies. The objective of the present study was to experimentally evaluate a hypothesis: an increased muscle tone promotes the use of ankle strategies. Research question: Do changes in the muscle tone affect the use of ankle strategies ?” 23
EXAMPLES OF HYPOTHESES IN PUBLISHED ARTICLES
- EXAMPLE 1. Working hypothesis (quantitative research)
- - A hypothesis that is initially accepted for further research to produce a feasible theory
- “As fever may have benefit in shortening the duration of viral illness, it is plausible to hypothesize that the antipyretic efficacy of ibuprofen may be hindering the benefits of a fever response when taken during the early stages of COVID-19 illness .” 24
- “In conclusion, it is plausible to hypothesize that the antipyretic efficacy of ibuprofen may be hindering the benefits of a fever response . The difference in perceived safety of these agents in COVID-19 illness could be related to the more potent efficacy to reduce fever with ibuprofen compared to acetaminophen. Compelling data on the benefit of fever warrant further research and review to determine when to treat or withhold ibuprofen for early stage fever for COVID-19 and other related viral illnesses .” 24
- EXAMPLE 2. Exploratory hypothesis (qualitative research)
- - Explores particular areas deeper to clarify subjective experience and develop a formal hypothesis potentially testable in a future quantitative approach
- “We hypothesized that when thinking about a past experience of help-seeking, a self distancing prompt would cause increased help-seeking intentions and more favorable help-seeking outcome expectations .” 25
- “Conclusion
- Although a priori hypotheses were not supported, further research is warranted as results indicate the potential for using self-distancing approaches to increasing help-seeking among some people with depressive symptomatology.” 25
- EXAMPLE 3. Hypothesis-generating research to establish a framework for hypothesis testing (qualitative research)
- “We hypothesize that compassionate care is beneficial for patients (better outcomes), healthcare systems and payers (lower costs), and healthcare providers (lower burnout). ” 26
- Compassionomics is the branch of knowledge and scientific study of the effects of compassionate healthcare. Our main hypotheses are that compassionate healthcare is beneficial for (1) patients, by improving clinical outcomes, (2) healthcare systems and payers, by supporting financial sustainability, and (3) HCPs, by lowering burnout and promoting resilience and well-being. The purpose of this paper is to establish a scientific framework for testing the hypotheses above . If these hypotheses are confirmed through rigorous research, compassionomics will belong in the science of evidence-based medicine, with major implications for all healthcare domains.” 26
- EXAMPLE 4. Statistical hypothesis (quantitative research)
- - An assumption is made about the relationship among several population characteristics ( gender differences in sociodemographic and clinical characteristics of adults with ADHD ). Validity is tested by statistical experiment or analysis ( chi-square test, Students t-test, and logistic regression analysis)
- “Our research investigated gender differences in sociodemographic and clinical characteristics of adults with ADHD in a Japanese clinical sample. Due to unique Japanese cultural ideals and expectations of women's behavior that are in opposition to ADHD symptoms, we hypothesized that women with ADHD experience more difficulties and present more dysfunctions than men . We tested the following hypotheses: first, women with ADHD have more comorbidities than men with ADHD; second, women with ADHD experience more social hardships than men, such as having less full-time employment and being more likely to be divorced.” 27
- “Statistical Analysis
- ( text omitted ) Between-gender comparisons were made using the chi-squared test for categorical variables and Students t-test for continuous variables…( text omitted ). A logistic regression analysis was performed for employment status, marital status, and comorbidity to evaluate the independent effects of gender on these dependent variables.” 27
EXAMPLES OF HYPOTHESIS AS WRITTEN IN PUBLISHED ARTICLES IN RELATION TO OTHER PARTS
- EXAMPLE 1. Background, hypotheses, and aims are provided
- “Pregnant women need skilled care during pregnancy and childbirth, but that skilled care is often delayed in some countries …( text omitted ). The focused antenatal care (FANC) model of WHO recommends that nurses provide information or counseling to all pregnant women …( text omitted ). Job aids are visual support materials that provide the right kind of information using graphics and words in a simple and yet effective manner. When nurses are not highly trained or have many work details to attend to, these job aids can serve as a content reminder for the nurses and can be used for educating their patients (Jennings, Yebadokpo, Affo, & Agbogbe, 2010) ( text omitted ). Importantly, additional evidence is needed to confirm how job aids can further improve the quality of ANC counseling by health workers in maternal care …( text omitted )” 28
- “ This has led us to hypothesize that the quality of ANC counseling would be better if supported by job aids. Consequently, a better quality of ANC counseling is expected to produce higher levels of awareness concerning the danger signs of pregnancy and a more favorable impression of the caring behavior of nurses .” 28
- “This study aimed to examine the differences in the responses of pregnant women to a job aid-supported intervention during ANC visit in terms of 1) their understanding of the danger signs of pregnancy and 2) their impression of the caring behaviors of nurses to pregnant women in rural Tanzania.” 28
- EXAMPLE 2. Background, hypotheses, and aims are provided
- “We conducted a two-arm randomized controlled trial (RCT) to evaluate and compare changes in salivary cortisol and oxytocin levels of first-time pregnant women between experimental and control groups. The women in the experimental group touched and held an infant for 30 min (experimental intervention protocol), whereas those in the control group watched a DVD movie of an infant (control intervention protocol). The primary outcome was salivary cortisol level and the secondary outcome was salivary oxytocin level.” 29
- “ We hypothesize that at 30 min after touching and holding an infant, the salivary cortisol level will significantly decrease and the salivary oxytocin level will increase in the experimental group compared with the control group .” 29
- EXAMPLE 3. Background, aim, and hypothesis are provided
- “In countries where the maternal mortality ratio remains high, antenatal education to increase Birth Preparedness and Complication Readiness (BPCR) is considered one of the top priorities [1]. BPCR includes birth plans during the antenatal period, such as the birthplace, birth attendant, transportation, health facility for complications, expenses, and birth materials, as well as family coordination to achieve such birth plans. In Tanzania, although increasing, only about half of all pregnant women attend an antenatal clinic more than four times [4]. Moreover, the information provided during antenatal care (ANC) is insufficient. In the resource-poor settings, antenatal group education is a potential approach because of the limited time for individual counseling at antenatal clinics.” 30
- “This study aimed to evaluate an antenatal group education program among pregnant women and their families with respect to birth-preparedness and maternal and infant outcomes in rural villages of Tanzania.” 30
- “ The study hypothesis was if Tanzanian pregnant women and their families received a family-oriented antenatal group education, they would (1) have a higher level of BPCR, (2) attend antenatal clinic four or more times, (3) give birth in a health facility, (4) have less complications of women at birth, and (5) have less complications and deaths of infants than those who did not receive the education .” 30
Research questions and hypotheses are crucial components to any type of research, whether quantitative or qualitative. These questions should be developed at the very beginning of the study. Excellent research questions lead to superior hypotheses, which, like a compass, set the direction of research, and can often determine the successful conduct of the study. Many research studies have floundered because the development of research questions and subsequent hypotheses was not given the thought and meticulous attention needed. The development of research questions and hypotheses is an iterative process based on extensive knowledge of the literature and insightful grasp of the knowledge gap. Focused, concise, and specific research questions provide a strong foundation for constructing hypotheses which serve as formal predictions about the research outcomes. Research questions and hypotheses are crucial elements of research that should not be overlooked. They should be carefully thought of and constructed when planning research. This avoids unethical studies and poor outcomes by defining well-founded objectives that determine the design, course, and outcome of the study.
Disclosure: The authors have no potential conflicts of interest to disclose.
Author Contributions:
- Conceptualization: Barroga E, Matanguihan GJ.
- Methodology: Barroga E, Matanguihan GJ.
- Writing - original draft: Barroga E, Matanguihan GJ.
- Writing - review & editing: Barroga E, Matanguihan GJ.
Ohio State nav bar
The Ohio State University
- BuckeyeLink
- Find People
- Search Ohio State
Research Questions & Hypotheses
Generally, in quantitative studies, reviewers expect hypotheses rather than research questions. However, both research questions and hypotheses serve different purposes and can be beneficial when used together.
Research Questions
Clarify the research’s aim (farrugia et al., 2010).
- Research often begins with an interest in a topic, but a deep understanding of the subject is crucial to formulate an appropriate research question.
- Descriptive: “What factors most influence the academic achievement of senior high school students?”
- Comparative: “What is the performance difference between teaching methods A and B?”
- Relationship-based: “What is the relationship between self-efficacy and academic achievement?”
- Increasing knowledge about a subject can be achieved through systematic literature reviews, in-depth interviews with patients (and proxies), focus groups, and consultations with field experts.
- Some funding bodies, like the Canadian Institute for Health Research, recommend conducting a systematic review or a pilot study before seeking grants for full trials.
- The presence of multiple research questions in a study can complicate the design, statistical analysis, and feasibility.
- It’s advisable to focus on a single primary research question for the study.
- The primary question, clearly stated at the end of a grant proposal’s introduction, usually specifies the study population, intervention, and other relevant factors.
- The FINER criteria underscore aspects that can enhance the chances of a successful research project, including specifying the population of interest, aligning with scientific and public interest, clinical relevance, and contribution to the field, while complying with ethical and national research standards.
| Feasible | ||
| Interesting | ||
| Novel | ||
| Ethical | ||
| Relevant |
- The P ICOT approach is crucial in developing the study’s framework and protocol, influencing inclusion and exclusion criteria and identifying patient groups for inclusion.
| Population (patients) | ||
| Intervention (for intervention studies only) | ||
| Comparison group | ||
| Outcome of interest | ||
| Time |
- Defining the specific population, intervention, comparator, and outcome helps in selecting the right outcome measurement tool.
- The more precise the population definition and stricter the inclusion and exclusion criteria, the more significant the impact on the interpretation, applicability, and generalizability of the research findings.
- A restricted study population enhances internal validity but may limit the study’s external validity and generalizability to clinical practice.
- A broadly defined study population may better reflect clinical practice but could increase bias and reduce internal validity.
- An inadequately formulated research question can negatively impact study design, potentially leading to ineffective outcomes and affecting publication prospects.
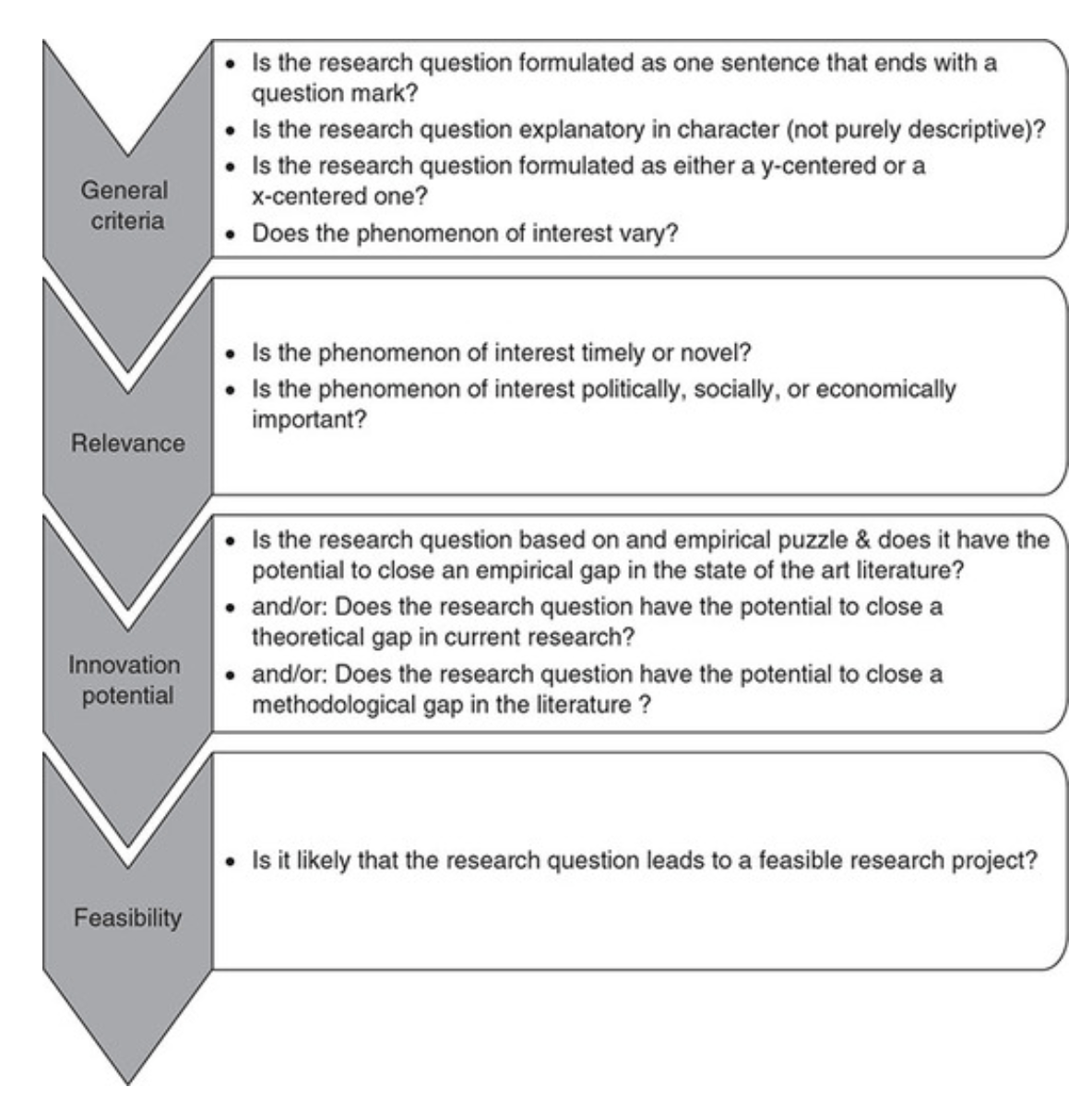
Checklist: Good research questions for social science projects (Panke, 2018)
Research Hypotheses
Present the researcher’s predictions based on specific statements.
- These statements define the research problem or issue and indicate the direction of the researcher’s predictions.
- Formulating the research question and hypothesis from existing data (e.g., a database) can lead to multiple statistical comparisons and potentially spurious findings due to chance.
- The research or clinical hypothesis, derived from the research question, shapes the study’s key elements: sampling strategy, intervention, comparison, and outcome variables.
- Hypotheses can express a single outcome or multiple outcomes.
- After statistical testing, the null hypothesis is either rejected or not rejected based on whether the study’s findings are statistically significant.
- Hypothesis testing helps determine if observed findings are due to true differences and not chance.
- Hypotheses can be 1-sided (specific direction of difference) or 2-sided (presence of a difference without specifying direction).
- 2-sided hypotheses are generally preferred unless there’s a strong justification for a 1-sided hypothesis.
- A solid research hypothesis, informed by a good research question, influences the research design and paves the way for defining clear research objectives.
Types of Research Hypothesis
- In a Y-centered research design, the focus is on the dependent variable (DV) which is specified in the research question. Theories are then used to identify independent variables (IV) and explain their causal relationship with the DV.
- Example: “An increase in teacher-led instructional time (IV) is likely to improve student reading comprehension scores (DV), because extensive guided practice under expert supervision enhances learning retention and skill mastery.”
- Hypothesis Explanation: The dependent variable (student reading comprehension scores) is the focus, and the hypothesis explores how changes in the independent variable (teacher-led instructional time) affect it.
- In X-centered research designs, the independent variable is specified in the research question. Theories are used to determine potential dependent variables and the causal mechanisms at play.
- Example: “Implementing technology-based learning tools (IV) is likely to enhance student engagement in the classroom (DV), because interactive and multimedia content increases student interest and participation.”
- Hypothesis Explanation: The independent variable (technology-based learning tools) is the focus, with the hypothesis exploring its impact on a potential dependent variable (student engagement).
- Probabilistic hypotheses suggest that changes in the independent variable are likely to lead to changes in the dependent variable in a predictable manner, but not with absolute certainty.
- Example: “The more teachers engage in professional development programs (IV), the more their teaching effectiveness (DV) is likely to improve, because continuous training updates pedagogical skills and knowledge.”
- Hypothesis Explanation: This hypothesis implies a probable relationship between the extent of professional development (IV) and teaching effectiveness (DV).
- Deterministic hypotheses state that a specific change in the independent variable will lead to a specific change in the dependent variable, implying a more direct and certain relationship.
- Example: “If the school curriculum changes from traditional lecture-based methods to project-based learning (IV), then student collaboration skills (DV) are expected to improve because project-based learning inherently requires teamwork and peer interaction.”
- Hypothesis Explanation: This hypothesis presumes a direct and definite outcome (improvement in collaboration skills) resulting from a specific change in the teaching method.
- Example : “Students who identify as visual learners will score higher on tests that are presented in a visually rich format compared to tests presented in a text-only format.”
- Explanation : This hypothesis aims to describe the potential difference in test scores between visual learners taking visually rich tests and text-only tests, without implying a direct cause-and-effect relationship.
- Example : “Teaching method A will improve student performance more than method B.”
- Explanation : This hypothesis compares the effectiveness of two different teaching methods, suggesting that one will lead to better student performance than the other. It implies a direct comparison but does not necessarily establish a causal mechanism.
- Example : “Students with higher self-efficacy will show higher levels of academic achievement.”
- Explanation : This hypothesis predicts a relationship between the variable of self-efficacy and academic achievement. Unlike a causal hypothesis, it does not necessarily suggest that one variable causes changes in the other, but rather that they are related in some way.
Tips for developing research questions and hypotheses for research studies
- Perform a systematic literature review (if one has not been done) to increase knowledge and familiarity with the topic and to assist with research development.
- Learn about current trends and technological advances on the topic.
- Seek careful input from experts, mentors, colleagues, and collaborators to refine your research question as this will aid in developing the research question and guide the research study.
- Use the FINER criteria in the development of the research question.
- Ensure that the research question follows PICOT format.
- Develop a research hypothesis from the research question.
- Ensure that the research question and objectives are answerable, feasible, and clinically relevant.
If your research hypotheses are derived from your research questions, particularly when multiple hypotheses address a single question, it’s recommended to use both research questions and hypotheses. However, if this isn’t the case, using hypotheses over research questions is advised. It’s important to note these are general guidelines, not strict rules. If you opt not to use hypotheses, consult with your supervisor for the best approach.
Farrugia, P., Petrisor, B. A., Farrokhyar, F., & Bhandari, M. (2010). Practical tips for surgical research: Research questions, hypotheses and objectives. Canadian journal of surgery. Journal canadien de chirurgie , 53 (4), 278–281.
Hulley, S. B., Cummings, S. R., Browner, W. S., Grady, D., & Newman, T. B. (2007). Designing clinical research. Philadelphia.
Panke, D. (2018). Research design & method selection: Making good choices in the social sciences. Research Design & Method Selection , 1-368.
How to Write a Research Question: Types and Examples

The first step in any research project is framing the research question. It can be considered the core of any systematic investigation as the research outcomes are tied to asking the right questions. Thus, this primary interrogation point sets the pace for your research as it helps collect relevant and insightful information that ultimately influences your work.
Typically, the research question guides the stages of inquiry, analysis, and reporting. Depending on the use of quantifiable or quantitative data, research questions are broadly categorized into quantitative or qualitative research questions. Both types of research questions can be used independently or together, considering the overall focus and objectives of your research.
What is a research question?
A research question is a clear, focused, concise, and arguable question on which your research and writing are centered. 1 It states various aspects of the study, including the population and variables to be studied and the problem the study addresses. These questions also set the boundaries of the study, ensuring cohesion.
Designing the research question is a dynamic process where the researcher can change or refine the research question as they review related literature and develop a framework for the study. Depending on the scale of your research, the study can include single or multiple research questions.
A good research question has the following features:
- It is relevant to the chosen field of study.
- The question posed is arguable and open for debate, requiring synthesizing and analysis of ideas.
- It is focused and concisely framed.
- A feasible solution is possible within the given practical constraint and timeframe.
A poorly formulated research question poses several risks. 1
- Researchers can adopt an erroneous design.
- It can create confusion and hinder the thought process, including developing a clear protocol.
- It can jeopardize publication efforts.
- It causes difficulty in determining the relevance of the study findings.
- It causes difficulty in whether the study fulfils the inclusion criteria for systematic review and meta-analysis. This creates challenges in determining whether additional studies or data collection is needed to answer the question.
- Readers may fail to understand the objective of the study. This reduces the likelihood of the study being cited by others.
Now that you know “What is a research question?”, let’s look at the different types of research questions.
Types of research questions
Depending on the type of research to be done, research questions can be classified broadly into quantitative, qualitative, or mixed-methods studies. Knowing the type of research helps determine the best type of research question that reflects the direction and epistemological underpinnings of your research.
The structure and wording of quantitative 2 and qualitative research 3 questions differ significantly. The quantitative study looks at causal relationships, whereas the qualitative study aims at exploring a phenomenon.
- Quantitative research questions:
- Seeks to investigate social, familial, or educational experiences or processes in a particular context and/or location.
- Answers ‘how,’ ‘what,’ or ‘why’ questions.
- Investigates connections, relations, or comparisons between independent and dependent variables.
Quantitative research questions can be further categorized into descriptive, comparative, and relationship, as explained in the Table below.
| Descriptive research questions | These measure the responses of a study’s population toward a particular question or variable. Common descriptive research questions will begin with “How much?”, “How regularly?”, “What percentage?”, “What time?”, “What is?” Research question example: How often do you buy mobile apps for learning purposes? |
| Comparative research questions | These investigate differences between two or more groups for an outcome variable. For instance, the researcher may compare groups with and without a certain variable. Research question example: What are the differences in attitudes towards online learning between visual and Kinaesthetic learners? |
| Relationship research questions | These explore and define trends and interactions between two or more variables. These investigate relationships between dependent and independent variables and use words such as “association” or “trends. Research question example: What is the relationship between disposable income and job satisfaction amongst US residents? |
- Qualitative research questions
Qualitative research questions are adaptable, non-directional, and more flexible. It concerns broad areas of research or more specific areas of study to discover, explain, or explore a phenomenon. These are further classified as follows:
| Exploratory Questions | These question looks to understand something without influencing the results. The aim is to learn more about a topic without attributing bias or preconceived notions. Research question example: What are people’s thoughts on the new government? |
| Experiential questions | These questions focus on understanding individuals’ experiences, perspectives, and subjective meanings related to a particular phenomenon. They aim to capture personal experiences and emotions. Research question example: What are the challenges students face during their transition from school to college? |
| Interpretive Questions | These questions investigate people in their natural settings to help understand how a group makes sense of shared experiences of a phenomenon. Research question example: How do you feel about ChatGPT assisting student learning? |
- Mixed-methods studies
Mixed-methods studies use both quantitative and qualitative research questions to answer your research question. Mixed methods provide a complete picture than standalone quantitative or qualitative research, as it integrates the benefits of both methods. Mixed methods research is often used in multidisciplinary settings and complex situational or societal research, especially in the behavioral, health, and social science fields.
What makes a good research question
A good research question should be clear and focused to guide your research. It should synthesize multiple sources to present your unique argument, and should ideally be something that you are interested in. But avoid questions that can be answered in a few factual statements. The following are the main attributes of a good research question.
- Specific: The research question should not be a fishing expedition performed in the hopes that some new information will be found that will benefit the researcher. The central research question should work with your research problem to keep your work focused. If using multiple questions, they should all tie back to the central aim.
- Measurable: The research question must be answerable using quantitative and/or qualitative data or from scholarly sources to develop your research question. If such data is impossible to access, it is better to rethink your question.
- Attainable: Ensure you have enough time and resources to do all research required to answer your question. If it seems you will not be able to gain access to the data you need, consider narrowing down your question to be more specific.
- You have the expertise
- You have the equipment and resources
- Realistic: Developing your research question should be based on initial reading about your topic. It should focus on addressing a problem or gap in the existing knowledge in your field or discipline.
- Based on some sort of rational physics
- Can be done in a reasonable time frame
- Timely: The research question should contribute to an existing and current debate in your field or in society at large. It should produce knowledge that future researchers or practitioners can later build on.
- Novel
- Based on current technologies.
- Important to answer current problems or concerns.
- Lead to new directions.
- Important: Your question should have some aspect of originality. Incremental research is as important as exploring disruptive technologies. For example, you can focus on a specific location or explore a new angle.
- Meaningful whether the answer is “Yes” or “No.” Closed-ended, yes/no questions are too simple to work as good research questions. Such questions do not provide enough scope for robust investigation and discussion. A good research question requires original data, synthesis of multiple sources, and original interpretation and argumentation before providing an answer.
Steps for developing a good research question
The importance of research questions cannot be understated. When drafting a research question, use the following frameworks to guide the components of your question to ease the process. 4
- Determine the requirements: Before constructing a good research question, set your research requirements. What is the purpose? Is it descriptive, comparative, or explorative research? Determining the research aim will help you choose the most appropriate topic and word your question appropriately.
- Select a broad research topic: Identify a broader subject area of interest that requires investigation. Techniques such as brainstorming or concept mapping can help identify relevant connections and themes within a broad research topic. For example, how to learn and help students learn.
- Perform preliminary investigation: Preliminary research is needed to obtain up-to-date and relevant knowledge on your topic. It also helps identify issues currently being discussed from which information gaps can be identified.
- Narrow your focus: Narrow the scope and focus of your research to a specific niche. This involves focusing on gaps in existing knowledge or recent literature or extending or complementing the findings of existing literature. Another approach involves constructing strong research questions that challenge your views or knowledge of the area of study (Example: Is learning consistent with the existing learning theory and research).
- Identify the research problem: Once the research question has been framed, one should evaluate it. This is to realize the importance of the research questions and if there is a need for more revising (Example: How do your beliefs on learning theory and research impact your instructional practices).
How to write a research question
Those struggling to understand how to write a research question, these simple steps can help you simplify the process of writing a research question.
| Topic selection | Choose a broad topic, such as “learner support” or “social media influence” for your study. Select topics of interest to make research more enjoyable and stay motivated. |
| Preliminary research | The goal is to refine and focus your research question. The following strategies can help: Skim various scholarly articles. List subtopics under the main topic. List possible research questions for each subtopic. Consider the scope of research for each of the research questions. Select research questions that are answerable within a specific time and with available resources. If the scope is too large, repeat looking for sub-subtopics. |
| Audience | When choosing what to base your research on, consider your readers. For college papers, the audience is academic. Ask yourself if your audience may be interested in the topic you are thinking about pursuing. Determining your audience can also help refine the importance of your research question and focus on items related to your defined group. |
| Generate potential questions | Ask open-ended “how?” and “why?” questions to find a more specific research question. Gap-spotting to identify research limitations, problematization to challenge assumptions made by others, or using personal experiences to draw on issues in your industry can be used to generate questions. |
| Review brainstormed questions | Evaluate each question to check their effectiveness. Use the FINER model to see if the question meets all the research question criteria. |
| Construct the research question | Multiple frameworks, such as PICOT and PEA, are available to help structure your research question. The frameworks listed below can help you with the necessary information for generating your research question. |
| Framework | Attributes of each framework |
| FINER | Feasible Interesting Novel Ethical Relevant |
| PICOT | Population or problem Intervention or indicator being studied Comparison group Outcome of interest Time frame of the study |
| PEO | Population being studied Exposure to preexisting conditions Outcome of interest |
Sample Research Questions
The following are some bad and good research question examples
- Example 1
| Unclear: How does social media affect student growth? |
| Clear: What effect does the daily use of Twitter and Facebook have on the career development goals of students? |
| Explanation: The first research question is unclear because of the vagueness of “social media” as a concept and the lack of specificity. The second question is specific and focused, and its answer can be discovered through data collection and analysis. |
- Example 2
| Simple: Has there been an increase in the number of gifted children identified? |
| Complex: What practical techniques can teachers use to identify and guide gifted children better? |
| Explanation: A simple “yes” or “no” statement easily answers the first research question. The second research question is more complicated and requires the researcher to collect data, perform in-depth data analysis, and form an argument that leads to further discussion. |
References:
- Thabane, L., Thomas, T., Ye, C., & Paul, J. (2009). Posing the research question: not so simple. Canadian Journal of Anesthesia/Journal canadien d’anesthésie , 56 (1), 71-79.
- Rutberg, S., & Bouikidis, C. D. (2018). Focusing on the fundamentals: A simplistic differentiation between qualitative and quantitative research. Nephrology Nursing Journal , 45 (2), 209-213.
- Kyngäs, H. (2020). Qualitative research and content analysis. The application of content analysis in nursing science research , 3-11.
- Mattick, K., Johnston, J., & de la Croix, A. (2018). How to… write a good research question. The clinical teacher , 15 (2), 104-108.
- Fandino, W. (2019). Formulating a good research question: Pearls and pitfalls. Indian Journal of Anaesthesia , 63 (8), 611.
- Richardson, W. S., Wilson, M. C., Nishikawa, J., & Hayward, R. S. (1995). The well-built clinical question: a key to evidence-based decisions. ACP journal club , 123 (3), A12-A13
Paperpal is a comprehensive AI writing toolkit that helps students and researchers achieve 2x the writing in half the time. It leverages 21+ years of STM experience and insights from millions of research articles to provide in-depth academic writing, language editing, and submission readiness support to help you write better, faster.
Get accurate academic translations, rewriting support, grammar checks, vocabulary suggestions, and generative AI assistance that delivers human precision at machine speed. Try for free or upgrade to Paperpal Prime starting at US$19 a month to access premium features, including consistency, plagiarism, and 30+ submission readiness checks to help you succeed.
Experience the future of academic writing – Sign up to Paperpal and start writing for free!
Related Reads:
- Scientific Writing Style Guides Explained
- Ethical Research Practices For Research with Human Subjects
- 8 Most Effective Ways to Increase Motivation for Thesis Writing
- 6 Tips for Post-Doc Researchers to Take Their Career to the Next Level
Transitive and Intransitive Verbs in the World of Research
Language and grammar rules for academic writing, you may also like, how to cite in apa format (7th edition):..., how to write your research paper in apa..., how to choose a dissertation topic, how to write a phd research proposal, how to write an academic paragraph (step-by-step guide), research funding basics: what should a grant proposal..., how to write the first draft of a..., mla works cited page: format, template & examples, academic editing: how to self-edit academic text with..., measuring academic success: definition & strategies for excellence.
- Research Questions: Definitions, Types + [Examples]

Research questions lie at the core of systematic investigation and this is because recording accurate research outcomes is tied to asking the right questions. Asking the right questions when conducting research can help you collect relevant and insightful information that ultimately influences your work, positively.
The right research questions are typically easy to understand, straight to the point, and engaging. In this article, we will share tips on how to create the right research questions and also show you how to create and administer an online questionnaire with Formplus .
What is a Research Question?
A research question is a specific inquiry which the research seeks to provide a response to. It resides at the core of systematic investigation and it helps you to clearly define a path for the research process.
A research question is usually the first step in any research project. Basically, it is the primary interrogation point of your research and it sets the pace for your work.
Typically, a research question focuses on the research, determines the methodology and hypothesis, and guides all stages of inquiry, analysis, and reporting. With the right research questions, you will be able to gather useful information for your investigation.
Types of Research Questions
Research questions are broadly categorized into 2; that is, qualitative research questions and quantitative research questions. Qualitative and quantitative research questions can be used independently and co-dependently in line with the overall focus and objectives of your research.
If your research aims at collecting quantifiable data , you will need to make use of quantitative research questions. On the other hand, qualitative questions help you to gather qualitative data bothering on the perceptions and observations of your research subjects.
Qualitative Research Questions
A qualitative research question is a type of systematic inquiry that aims at collecting qualitative data from research subjects. The aim of qualitative research questions is to gather non-statistical information pertaining to the experiences, observations, and perceptions of the research subjects in line with the objectives of the investigation.
Types of Qualitative Research Questions
- Ethnographic Research Questions
As the name clearly suggests, ethnographic research questions are inquiries presented in ethnographic research. Ethnographic research is a qualitative research approach that involves observing variables in their natural environments or habitats in order to arrive at objective research outcomes.
These research questions help the researcher to gather insights into the habits, dispositions, perceptions, and behaviors of research subjects as they interact in specific environments.
Ethnographic research questions can be used in education, business, medicine, and other fields of study, and they are very useful in contexts aimed at collecting in-depth and specific information that are peculiar to research variables. For instance, asking educational ethnographic research questions can help you understand how pedagogy affects classroom relations and behaviors.
This type of research question can be administered physically through one-on-one interviews, naturalism (live and work), and participant observation methods. Alternatively, the researcher can ask ethnographic research questions via online surveys and questionnaires created with Formplus.
Examples of Ethnographic Research Questions
- Why do you use this product?
- Have you noticed any side effects since you started using this drug?
- Does this product meet your needs?

- Case Studies
A case study is a qualitative research approach that involves carrying out a detailed investigation into a research subject(s) or variable(s). In the course of a case study, the researcher gathers a range of data from multiple sources of information via different data collection methods, and over a period of time.
The aim of a case study is to analyze specific issues within definite contexts and arrive at detailed research subject analyses by asking the right questions. This research method can be explanatory, descriptive , or exploratory depending on the focus of your systematic investigation or research.
An explanatory case study is one that seeks to gather information on the causes of real-life occurrences. This type of case study uses “how” and “why” questions in order to gather valid information about the causative factors of an event.
Descriptive case studies are typically used in business researches, and they aim at analyzing the impact of changing market dynamics on businesses. On the other hand, exploratory case studies aim at providing answers to “who” and “what” questions using data collection tools like interviews and questionnaires.
Some questions you can include in your case studies are:
- Why did you choose our services?
- How has this policy affected your business output?
- What benefits have you recorded since you started using our product?

An interview is a qualitative research method that involves asking respondents a series of questions in order to gather information about a research subject. Interview questions can be close-ended or open-ended , and they prompt participants to provide valid information that is useful to the research.
An interview may also be structured, semi-structured , or unstructured , and this further influences the types of questions they include. Structured interviews are made up of more close-ended questions because they aim at gathering quantitative data while unstructured interviews consist, primarily, of open-ended questions that allow the researcher to collect qualitative information from respondents.
You can conduct interview research by scheduling a physical meeting with respondents, through a telephone conversation, and via digital media and video conferencing platforms like Skype and Zoom. Alternatively, you can use Formplus surveys and questionnaires for your interview.
Examples of interview questions include:
- What challenges did you face while using our product?
- What specific needs did our product meet?
- What would you like us to improve our service delivery?

Quantitative Research Questions
Quantitative research questions are questions that are used to gather quantifiable data from research subjects. These types of research questions are usually more specific and direct because they aim at collecting information that can be measured; that is, statistical information.
Types of Quantitative Research Questions
- Descriptive Research Questions
Descriptive research questions are inquiries that researchers use to gather quantifiable data about the attributes and characteristics of research subjects. These types of questions primarily seek responses that reveal existing patterns in the nature of the research subjects.
It is important to note that descriptive research questions are not concerned with the causative factors of the discovered attributes and characteristics. Rather, they focus on the “what”; that is, describing the subject of the research without paying attention to the reasons for its occurrence.
Descriptive research questions are typically closed-ended because they aim at gathering definite and specific responses from research participants. Also, they can be used in customer experience surveys and market research to collect information about target markets and consumer behaviors.
Descriptive Research Question Examples
- How often do you make use of our fitness application?
- How much would you be willing to pay for this product?

- Comparative Research Questions
A comparative research question is a type of quantitative research question that is used to gather information about the differences between two or more research subjects across different variables. These types of questions help the researcher to identify distinct features that mark one research subject from the other while highlighting existing similarities.
Asking comparative research questions in market research surveys can provide insights on how your product or service matches its competitors. In addition, it can help you to identify the strengths and weaknesses of your product for a better competitive advantage.
The 5 steps involved in the framing of comparative research questions are:
- Choose your starting phrase
- Identify and name the dependent variable
- Identify the groups you are interested in
- Identify the appropriate adjoining text
- Write out the comparative research question
Comparative Research Question Samples
- What are the differences between a landline telephone and a smartphone?
- What are the differences between work-from-home and on-site operations?

- Relationship-based Research Questions
Just like the name suggests, a relationship-based research question is one that inquires into the nature of the association between two research subjects within the same demographic. These types of research questions help you to gather information pertaining to the nature of the association between two research variables.
Relationship-based research questions are also known as correlational research questions because they seek to clearly identify the link between 2 variables.
Read: Correlational Research Designs: Types, Examples & Methods
Examples of relationship-based research questions include:
- What is the relationship between purchasing power and the business site?
- What is the relationship between the work environment and workforce turnover?

Examples of a Good Research Question
Since research questions lie at the core of any systematic investigations, it is important to know how to frame a good research question. The right research questions will help you to gather the most objective responses that are useful to your systematic investigation.
A good research question is one that requires impartial responses and can be answered via existing sources of information. Also, a good research question seeks answers that actively contribute to a body of knowledge; hence, it is a question that is yet to be answered in your specific research context.
- Open-Ended Questions
An open-ended question is a type of research question that does not restrict respondents to a set of premeditated answer options. In other words, it is a question that allows the respondent to freely express his or her perceptions and feelings towards the research subject.
Examples of Open-ended Questions
- How do you deal with stress in the workplace?
- What is a typical day at work like for you?
- Close-ended Questions
A close-ended question is a type of survey question that restricts respondents to a set of predetermined answers such as multiple-choice questions . Close-ended questions typically require yes or no answers and are commonly used in quantitative research to gather numerical data from research participants.
Examples of Close-ended Questions
- Did you enjoy this event?
- How likely are you to recommend our services?
- Very Likely
- Somewhat Likely
- Likert Scale Questions
A Likert scale question is a type of close-ended question that is structured as a 3-point, 5-point, or 7-point psychometric scale . This type of question is used to measure the survey respondent’s disposition towards multiple variables and it can be unipolar or bipolar in nature.
Example of Likert Scale Questions
- How satisfied are you with our service delivery?
- Very dissatisfied
- Not satisfied
- Very satisfied
- Rating Scale Questions
A rating scale question is a type of close-ended question that seeks to associate a specific qualitative measure (rating) with the different variables in research. It is commonly used in customer experience surveys, market research surveys, employee reviews, and product evaluations.
Example of Rating Questions
- How would you rate our service delivery?
Examples of a Bad Research Question
Knowing what bad research questions are would help you avoid them in the course of your systematic investigation. These types of questions are usually unfocused and often result in research biases that can negatively impact the outcomes of your systematic investigation.
- Loaded Questions
A loaded question is a question that subtly presupposes one or more unverified assumptions about the research subject or participant. This type of question typically boxes the respondent in a corner because it suggests implicit and explicit biases that prevent objective responses.
Example of Loaded Questions
- Have you stopped smoking?
- Where did you hide the money?
- Negative Questions
A negative question is a type of question that is structured with an implicit or explicit negator. Negative questions can be misleading because they upturn the typical yes/no response order by requiring a negative answer for affirmation and an affirmative answer for negation.
Examples of Negative Questions
- Would you mind dropping by my office later today?
- Didn’t you visit last week?
- Leading Questions
A l eading question is a type of survey question that nudges the respondent towards an already-determined answer. It is highly suggestive in nature and typically consists of biases and unverified assumptions that point toward its premeditated responses.
Examples of Leading Questions
- If you enjoyed this service, would you be willing to try out our other packages?
- Our product met your needs, didn’t it?
Read More: Leading Questions: Definition, Types, and Examples
How to Use Formplus as Online Research Questionnaire Tool
With Formplus, you can create and administer your online research questionnaire easily. In the form builder, you can add different form fields to your questionnaire and edit these fields to reflect specific research questions for your systematic investigation.
Here is a step-by-step guide on how to create an online research questionnaire with Formplus:
- Sign in to your Formplus accoun t, then click on the “create new form” button in your dashboard to access the Form builder.

- In the form builder, add preferred form fields to your online research questionnaire by dragging and dropping them into the form. Add a title to your form in the title block. You can edit form fields by clicking on the “pencil” icon on the right corner of each form field.

- Save the form to access the customization section of the builder. Here, you can tweak the appearance of your online research questionnaire by adding background images, changing the form font, and adding your organization’s logo.

- Finally, copy your form link and share it with respondents. You can also use any of the multiple sharing options available.

Conclusion
The success of your research starts with framing the right questions to help you collect the most valid and objective responses. Be sure to avoid bad research questions like loaded and negative questions that can be misleading and adversely affect your research data and outcomes.
Your research questions should clearly reflect the aims and objectives of your systematic investigation while laying emphasis on specific contexts. To help you seamlessly gather responses for your research questions, you can create an online research questionnaire on Formplus.
Connect to Formplus, Get Started Now - It's Free!
- abstract in research papers
- bad research questions
- examples of research questions
- types of research questions
- busayo.longe
You may also like:
How to Write An Abstract For Research Papers: Tips & Examples
In this article, we will share some tips for writing an effective abstract, plus samples you can learn from.
Research Summary: What Is It & How To Write One
Introduction A research summary is a requirement during academic research and sometimes you might need to prepare a research summary...
How to Write a Problem Statement for your Research
Learn how to write problem statements before commencing any research effort. Learn about its structure and explore examples
How to do a Meta Analysis: Methodology, Pros & Cons
In this article, we’ll go through the concept of meta-analysis, what it can be used for, and how you can use it to improve how you...
Formplus - For Seamless Data Collection
Collect data the right way with a versatile data collection tool. try formplus and transform your work productivity today..
Research Variables 101
Independent variables, dependent variables, control variables and more
By: Derek Jansen (MBA) | Expert Reviewed By: Kerryn Warren (PhD) | January 2023
If you’re new to the world of research, especially scientific research, you’re bound to run into the concept of variables , sooner or later. If you’re feeling a little confused, don’t worry – you’re not the only one! Independent variables, dependent variables, confounding variables – it’s a lot of jargon. In this post, we’ll unpack the terminology surrounding research variables using straightforward language and loads of examples .
Overview: Variables In Research
| 1. ? 2. variables 3. variables 4. variables | 5. variables |
What (exactly) is a variable?
The simplest way to understand a variable is as any characteristic or attribute that can experience change or vary over time or context – hence the name “variable”. For example, the dosage of a particular medicine could be classified as a variable, as the amount can vary (i.e., a higher dose or a lower dose). Similarly, gender, age or ethnicity could be considered demographic variables, because each person varies in these respects.
Within research, especially scientific research, variables form the foundation of studies, as researchers are often interested in how one variable impacts another, and the relationships between different variables. For example:
- How someone’s age impacts their sleep quality
- How different teaching methods impact learning outcomes
- How diet impacts weight (gain or loss)
As you can see, variables are often used to explain relationships between different elements and phenomena. In scientific studies, especially experimental studies, the objective is often to understand the causal relationships between variables. In other words, the role of cause and effect between variables. This is achieved by manipulating certain variables while controlling others – and then observing the outcome. But, we’ll get into that a little later…
The “Big 3” Variables
Variables can be a little intimidating for new researchers because there are a wide variety of variables, and oftentimes, there are multiple labels for the same thing. To lay a firm foundation, we’ll first look at the three main types of variables, namely:
- Independent variables (IV)
- Dependant variables (DV)
- Control variables
What is an independent variable?
Simply put, the independent variable is the “ cause ” in the relationship between two (or more) variables. In other words, when the independent variable changes, it has an impact on another variable.
For example:
- Increasing the dosage of a medication (Variable A) could result in better (or worse) health outcomes for a patient (Variable B)
- Changing a teaching method (Variable A) could impact the test scores that students earn in a standardised test (Variable B)
- Varying one’s diet (Variable A) could result in weight loss or gain (Variable B).
It’s useful to know that independent variables can go by a few different names, including, explanatory variables (because they explain an event or outcome) and predictor variables (because they predict the value of another variable). Terminology aside though, the most important takeaway is that independent variables are assumed to be the “cause” in any cause-effect relationship. As you can imagine, these types of variables are of major interest to researchers, as many studies seek to understand the causal factors behind a phenomenon.
Need a helping hand?
What is a dependent variable?
While the independent variable is the “ cause ”, the dependent variable is the “ effect ” – or rather, the affected variable . In other words, the dependent variable is the variable that is assumed to change as a result of a change in the independent variable.
Keeping with the previous example, let’s look at some dependent variables in action:
- Health outcomes (DV) could be impacted by dosage changes of a medication (IV)
- Students’ scores (DV) could be impacted by teaching methods (IV)
- Weight gain or loss (DV) could be impacted by diet (IV)
In scientific studies, researchers will typically pay very close attention to the dependent variable (or variables), carefully measuring any changes in response to hypothesised independent variables. This can be tricky in practice, as it’s not always easy to reliably measure specific phenomena or outcomes – or to be certain that the actual cause of the change is in fact the independent variable.
As the adage goes, correlation is not causation . In other words, just because two variables have a relationship doesn’t mean that it’s a causal relationship – they may just happen to vary together. For example, you could find a correlation between the number of people who own a certain brand of car and the number of people who have a certain type of job. Just because the number of people who own that brand of car and the number of people who have that type of job is correlated, it doesn’t mean that owning that brand of car causes someone to have that type of job or vice versa. The correlation could, for example, be caused by another factor such as income level or age group, which would affect both car ownership and job type.
To confidently establish a causal relationship between an independent variable and a dependent variable (i.e., X causes Y), you’ll typically need an experimental design , where you have complete control over the environmen t and the variables of interest. But even so, this doesn’t always translate into the “real world”. Simply put, what happens in the lab sometimes stays in the lab!
As an alternative to pure experimental research, correlational or “ quasi-experimental ” research (where the researcher cannot manipulate or change variables) can be done on a much larger scale more easily, allowing one to understand specific relationships in the real world. These types of studies also assume some causality between independent and dependent variables, but it’s not always clear. So, if you go this route, you need to be cautious in terms of how you describe the impact and causality between variables and be sure to acknowledge any limitations in your own research.

What is a control variable?
In an experimental design, a control variable (or controlled variable) is a variable that is intentionally held constant to ensure it doesn’t have an influence on any other variables. As a result, this variable remains unchanged throughout the course of the study. In other words, it’s a variable that’s not allowed to vary – tough life 🙂
As we mentioned earlier, one of the major challenges in identifying and measuring causal relationships is that it’s difficult to isolate the impact of variables other than the independent variable. Simply put, there’s always a risk that there are factors beyond the ones you’re specifically looking at that might be impacting the results of your study. So, to minimise the risk of this, researchers will attempt (as best possible) to hold other variables constant . These factors are then considered control variables.
Some examples of variables that you may need to control include:
- Temperature
- Time of day
- Noise or distractions
Which specific variables need to be controlled for will vary tremendously depending on the research project at hand, so there’s no generic list of control variables to consult. As a researcher, you’ll need to think carefully about all the factors that could vary within your research context and then consider how you’ll go about controlling them. A good starting point is to look at previous studies similar to yours and pay close attention to which variables they controlled for.
Of course, you won’t always be able to control every possible variable, and so, in many cases, you’ll just have to acknowledge their potential impact and account for them in the conclusions you draw. Every study has its limitations , so don’t get fixated or discouraged by troublesome variables. Nevertheless, always think carefully about the factors beyond what you’re focusing on – don’t make assumptions!

Other types of variables
As we mentioned, independent, dependent and control variables are the most common variables you’ll come across in your research, but they’re certainly not the only ones you need to be aware of. Next, we’ll look at a few “secondary” variables that you need to keep in mind as you design your research.
- Moderating variables
- Mediating variables
- Confounding variables
- Latent variables
Let’s jump into it…
What is a moderating variable?
A moderating variable is a variable that influences the strength or direction of the relationship between an independent variable and a dependent variable. In other words, moderating variables affect how much (or how little) the IV affects the DV, or whether the IV has a positive or negative relationship with the DV (i.e., moves in the same or opposite direction).
For example, in a study about the effects of sleep deprivation on academic performance, gender could be used as a moderating variable to see if there are any differences in how men and women respond to a lack of sleep. In such a case, one may find that gender has an influence on how much students’ scores suffer when they’re deprived of sleep.
It’s important to note that while moderators can have an influence on outcomes , they don’t necessarily cause them ; rather they modify or “moderate” existing relationships between other variables. This means that it’s possible for two different groups with similar characteristics, but different levels of moderation, to experience very different results from the same experiment or study design.
What is a mediating variable?
Mediating variables are often used to explain the relationship between the independent and dependent variable (s). For example, if you were researching the effects of age on job satisfaction, then education level could be considered a mediating variable, as it may explain why older people have higher job satisfaction than younger people – they may have more experience or better qualifications, which lead to greater job satisfaction.
Mediating variables also help researchers understand how different factors interact with each other to influence outcomes. For instance, if you wanted to study the effect of stress on academic performance, then coping strategies might act as a mediating factor by influencing both stress levels and academic performance simultaneously. For example, students who use effective coping strategies might be less stressed but also perform better academically due to their improved mental state.
In addition, mediating variables can provide insight into causal relationships between two variables by helping researchers determine whether changes in one factor directly cause changes in another – or whether there is an indirect relationship between them mediated by some third factor(s). For instance, if you wanted to investigate the impact of parental involvement on student achievement, you would need to consider family dynamics as a potential mediator, since it could influence both parental involvement and student achievement simultaneously.

What is a confounding variable?
A confounding variable (also known as a third variable or lurking variable ) is an extraneous factor that can influence the relationship between two variables being studied. Specifically, for a variable to be considered a confounding variable, it needs to meet two criteria:
- It must be correlated with the independent variable (this can be causal or not)
- It must have a causal impact on the dependent variable (i.e., influence the DV)
Some common examples of confounding variables include demographic factors such as gender, ethnicity, socioeconomic status, age, education level, and health status. In addition to these, there are also environmental factors to consider. For example, air pollution could confound the impact of the variables of interest in a study investigating health outcomes.
Naturally, it’s important to identify as many confounding variables as possible when conducting your research, as they can heavily distort the results and lead you to draw incorrect conclusions . So, always think carefully about what factors may have a confounding effect on your variables of interest and try to manage these as best you can.
What is a latent variable?
Latent variables are unobservable factors that can influence the behaviour of individuals and explain certain outcomes within a study. They’re also known as hidden or underlying variables , and what makes them rather tricky is that they can’t be directly observed or measured . Instead, latent variables must be inferred from other observable data points such as responses to surveys or experiments.
For example, in a study of mental health, the variable “resilience” could be considered a latent variable. It can’t be directly measured , but it can be inferred from measures of mental health symptoms, stress, and coping mechanisms. The same applies to a lot of concepts we encounter every day – for example:
- Emotional intelligence
- Quality of life
- Business confidence
- Ease of use
One way in which we overcome the challenge of measuring the immeasurable is latent variable models (LVMs). An LVM is a type of statistical model that describes a relationship between observed variables and one or more unobserved (latent) variables. These models allow researchers to uncover patterns in their data which may not have been visible before, thanks to their complexity and interrelatedness with other variables. Those patterns can then inform hypotheses about cause-and-effect relationships among those same variables which were previously unknown prior to running the LVM. Powerful stuff, we say!

Let’s recap
In the world of scientific research, there’s no shortage of variable types, some of which have multiple names and some of which overlap with each other. In this post, we’ve covered some of the popular ones, but remember that this is not an exhaustive list .
To recap, we’ve explored:
- Independent variables (the “cause”)
- Dependent variables (the “effect”)
- Control variables (the variable that’s not allowed to vary)
If you’re still feeling a bit lost and need a helping hand with your research project, check out our 1-on-1 coaching service , where we guide you through each step of the research journey. Also, be sure to check out our free dissertation writing course and our collection of free, fully-editable chapter templates .

Psst... there’s more!
This post was based on one of our popular Research Bootcamps . If you're working on a research project, you'll definitely want to check this out ...

Very informative, concise and helpful. Thank you

Helping information.Thanks

practical and well-demonstrated

Very helpful and insightful
Submit a Comment Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Print Friendly
Quantitative Research: Examples of Research Questions and Solutions
Are you ready to embark on a journey into the world of quantitative research? Whether you’re a seasoned researcher or just beginning your academic journey, understanding how to formulate effective research questions is essential for conducting meaningful studies. In this blog post, we’ll explore examples of quantitative research questions across various disciplines and discuss how StatsCamp.org courses can provide the tools and support you need to overcome any challenges you may encounter along the way.
Understanding Quantitative Research Questions
Quantitative research involves collecting and analyzing numerical data to answer research questions and test hypotheses. These questions typically seek to understand the relationships between variables, predict outcomes, or compare groups. Let’s explore some examples of quantitative research questions across different fields:

- What is the relationship between class size and student academic performance?
- Does the use of technology in the classroom improve learning outcomes?
- How does parental involvement affect student achievement?
- What is the effect of a new drug treatment on reducing blood pressure?
- Is there a correlation between physical activity levels and the risk of cardiovascular disease?
- How does socioeconomic status influence access to healthcare services?
- What factors influence consumer purchasing behavior?
- Is there a relationship between advertising expenditure and sales revenue?
- How do demographic variables affect brand loyalty?
Stats Camp: Your Solution to Mastering Quantitative Research Methodologies
At StatsCamp.org, we understand that navigating the complexities of quantitative research can be daunting. That’s why we offer a range of courses designed to equip you with the knowledge and skills you need to excel in your research endeavors. Whether you’re interested in learning about regression analysis, experimental design, or structural equation modeling, our experienced instructors are here to guide you every step of the way.
Bringing Your Own Data
One of the unique features of StatsCamp.org is the opportunity to bring your own data to the learning process. Our instructors provide personalized guidance and support to help you analyze your data effectively and overcome any roadblocks you may encounter. Whether you’re struggling with data cleaning, model specification, or interpretation of results, our team is here to help you succeed.
Courses Offered at StatsCamp.org
- Latent Profile Analysis Course : Learn how to identify subgroups, or profiles, within a heterogeneous population based on patterns of responses to multiple observed variables.
- Bayesian Statistics Course : A comprehensive introduction to Bayesian data analysis, a powerful statistical approach for inference and decision-making. Through a series of engaging lectures and hands-on exercises, participants will learn how to apply Bayesian methods to a wide range of research questions and data types.
- Structural Equation Modeling (SEM) Course : Dive into advanced statistical techniques for modeling complex relationships among variables.
- Multilevel Modeling Course : A in-depth exploration of this advanced statistical technique, designed to analyze data with nested structures or hierarchies. Whether you’re studying individuals within groups, schools within districts, or any other nested data structure, multilevel modeling provides the tools to account for the dependencies inherent in such data.
As you embark on your journey into quantitative research, remember that StatsCamp.org is here to support you every step of the way. Whether you’re formulating research questions, analyzing data, or interpreting results, our courses provide the knowledge and expertise you need to succeed. Join us today and unlock the power of quantitative research!
Follow Us On Social! Facebook | Instagram | X
933 San Mateo Blvd NE #500, Albuquerque, NM 87108
4414 82 nd Street #212-121 Lubbock, TX 79424
Monday – Friday: 9:00 AM – 5:00 PM
© Copyright 2003 - 2024 | All Rights Reserved Stats Camp Foundation 501(c)(3) Non-Profit Organization.
Statistical Research Questions: Five Examples for Quantitative Analysis
Table of contents, introduction.
How are statistical research questions for quantitative analysis written? This article provides five examples of statistical research questions that will allow statistical analysis to take place.
In quantitative research projects, writing statistical research questions requires a good understanding and the ability to discern the type of data that you will analyze. This knowledge is elemental in framing research questions that shall guide you in identifying the appropriate statistical test to use in your research.
Thus, before writing your statistical research questions and reading the examples in this article, read first the article that enumerates the four types of measurement scales . Knowing the four types of measurement scales will enable you to appreciate the formulation or structuring of research questions.
Five Examples of Statistical Research Questions
In writing the statistical research questions, I provide a topic that shows the variables of the study, the study description, and a link to the original scientific article to give you a glimpse of the real-world examples.
Topic 1: Physical Fitness and Academic Achievement
Statistical research question no. 1.
Is there a significant relationship between physical fitness and academic achievement?
On the other hand, the researchers measured academic achievement in terms of a passing score in Mathematics and English. The variable is the number of passing scores in both Mathematics and English.
In the particular study mentioned, the researchers used multivariate logistic regression analyses to assess the probability of passing the tests, controlling for students’ weight status, ethnicity, gender, grade, and socioeconomic status. For the novice researcher, this requires further study of multivariate (or many variables) statistical tests. You may study it on your own.
Most of what I discuss in the statistics articles I wrote came from self-study. It’s easier to understand concepts now as there are a lot of resource materials available online. Videos and ebooks from places like Youtube, Veoh, The Internet Archives, among others, provide free educational materials. Online education will be the norm of the future. I describe this situation in my post about Education 4.0 .
Topic 2: Climate Conditions and Consumption of Bottled Water
Statistical research question no. 2.
Is there a significant relationship between average temperature and amount of bottled water consumed?
Now, it’s easy to identify the statistical test to analyze the relationship between the two variables. You may refer to my previous post titled Parametric Statistics: Four Widely Used Parametric Tests and When to Use Them . Using the figure supplied in that article, the appropriate test to use is, again, Pearson’s Correlation Coefficient.
Topic 3: Nursing Home Staff Size and Number of COVID-19 Cases
Statistical research question no. 3.
Note that this study on COVID-19 looked into three variables, namely 1) number of unique employees working in skilled nursing homes, 2) number of weekly confirmed cases among residents and staff, and 3) number of weekly COVID-19 deaths among residents.
A simple Pearson test may be used to correlate one variable with another variable. But the study used multiple variables. Hence, they produced regression models that show how multiple variables affect the outcome. Some of the variables in the study may be redundant, meaning, those variables may represent the same attribute of a population. Stepwise multiple regression models take care of those redundancies. Using this statistical test requires further study and experience.
Topic 4: Surrounding Greenness, Stress, and Memory
Statistical research question no. 4.
As this article is behind a paywall and we cannot see the full article, we can content ourselves with the knowledge that three major variables were explored in this study. These are 1) exposure to and use of natural environments, 2) stress, and 3) memory performance.
Topic 5: Income and Happiness
This recent finding is an interesting read and is available online. Just click on the link I provide as the source below. The study sought to determine if income plays a role in people’s happiness across three age groups: young (18-30 years), middle (31-64 years), and old (65 or older). The literature review suggests that income has a positive effect on an individual’s sense of happiness. That’s because more money increases opportunities to fulfill dreams and buy more goods and services.
An investigation was conducted to determine if the size of nursing home staff and the number of COVID-19 cases are correlated. Specifically, they looked into the number of unique employees working daily, and the outcomes include weekly counts of confirmed COVID-19 cases among residents and staff and weekly COVID-19 deaths among residents.
Statistical Research Question No. 5
I do hope that upon reaching this part of the article, you are now well familiar on how to write statistical research questions. Practice makes perfect.
References:
Måseide, H. (2021). Income and Happiness: Does the relationship vary with age?
© P. A. Regoniel 12 October 2021 | Updated 08 January 2024
Related Posts
What is the difference between theory testing and theory building, heart rate analysis: example of t-test using ms excel analysis toolpak, honing research skills through self-study: 3 key ideas, about the author, patrick regoniel, simplyeducate.me privacy policy.
- Privacy Policy
Home » Research Questions – Types, Examples and Writing Guide
Research Questions – Types, Examples and Writing Guide
Table of Contents

Research Questions
Definition:
Research questions are the specific questions that guide a research study or inquiry. These questions help to define the scope of the research and provide a clear focus for the study. Research questions are usually developed at the beginning of a research project and are designed to address a particular research problem or objective.
Types of Research Questions
Types of Research Questions are as follows:
Descriptive Research Questions
These aim to describe a particular phenomenon, group, or situation. For example:
- What are the characteristics of the target population?
- What is the prevalence of a particular disease in a specific region?
Exploratory Research Questions
These aim to explore a new area of research or generate new ideas or hypotheses. For example:
- What are the potential causes of a particular phenomenon?
- What are the possible outcomes of a specific intervention?
Explanatory Research Questions
These aim to understand the relationship between two or more variables or to explain why a particular phenomenon occurs. For example:
- What is the effect of a specific drug on the symptoms of a particular disease?
- What are the factors that contribute to employee turnover in a particular industry?
Predictive Research Questions
These aim to predict a future outcome or trend based on existing data or trends. For example :
- What will be the future demand for a particular product or service?
- What will be the future prevalence of a particular disease?
Evaluative Research Questions
These aim to evaluate the effectiveness of a particular intervention or program. For example:
- What is the impact of a specific educational program on student learning outcomes?
- What is the effectiveness of a particular policy or program in achieving its intended goals?
How to Choose Research Questions
Choosing research questions is an essential part of the research process and involves careful consideration of the research problem, objectives, and design. Here are some steps to consider when choosing research questions:
- Identify the research problem: Start by identifying the problem or issue that you want to study. This could be a gap in the literature, a social or economic issue, or a practical problem that needs to be addressed.
- Conduct a literature review: Conducting a literature review can help you identify existing research in your area of interest and can help you formulate research questions that address gaps or limitations in the existing literature.
- Define the research objectives : Clearly define the objectives of your research. What do you want to achieve with your study? What specific questions do you want to answer?
- Consider the research design : Consider the research design that you plan to use. This will help you determine the appropriate types of research questions to ask. For example, if you plan to use a qualitative approach, you may want to focus on exploratory or descriptive research questions.
- Ensure that the research questions are clear and answerable: Your research questions should be clear and specific, and should be answerable with the data that you plan to collect. Avoid asking questions that are too broad or vague.
- Get feedback : Get feedback from your supervisor, colleagues, or peers to ensure that your research questions are relevant, feasible, and meaningful.
How to Write Research Questions
Guide for Writing Research Questions:
- Start with a clear statement of the research problem: Begin by stating the problem or issue that your research aims to address. This will help you to formulate focused research questions.
- Use clear language : Write your research questions in clear and concise language that is easy to understand. Avoid using jargon or technical terms that may be unfamiliar to your readers.
- Be specific: Your research questions should be specific and focused. Avoid broad questions that are difficult to answer. For example, instead of asking “What is the impact of climate change on the environment?” ask “What are the effects of rising sea levels on coastal ecosystems?”
- Use appropriate question types: Choose the appropriate question types based on the research design and objectives. For example, if you are conducting a qualitative study, you may want to use open-ended questions that allow participants to provide detailed responses.
- Consider the feasibility of your questions : Ensure that your research questions are feasible and can be answered with the resources available. Consider the data sources and methods of data collection when writing your questions.
- Seek feedback: Get feedback from your supervisor, colleagues, or peers to ensure that your research questions are relevant, appropriate, and meaningful.
Examples of Research Questions
Some Examples of Research Questions with Research Titles:
Research Title: The Impact of Social Media on Mental Health
- Research Question : What is the relationship between social media use and mental health, and how does this impact individuals’ well-being?
Research Title: Factors Influencing Academic Success in High School
- Research Question: What are the primary factors that influence academic success in high school, and how do they contribute to student achievement?
Research Title: The Effects of Exercise on Physical and Mental Health
- Research Question: What is the relationship between exercise and physical and mental health, and how can exercise be used as a tool to improve overall well-being?
Research Title: Understanding the Factors that Influence Consumer Purchasing Decisions
- Research Question : What are the key factors that influence consumer purchasing decisions, and how do these factors vary across different demographics and products?
Research Title: The Impact of Technology on Communication
- Research Question : How has technology impacted communication patterns, and what are the effects of these changes on interpersonal relationships and society as a whole?
Research Title: Investigating the Relationship between Parenting Styles and Child Development
- Research Question: What is the relationship between different parenting styles and child development outcomes, and how do these outcomes vary across different ages and developmental stages?
Research Title: The Effectiveness of Cognitive-Behavioral Therapy in Treating Anxiety Disorders
- Research Question: How effective is cognitive-behavioral therapy in treating anxiety disorders, and what factors contribute to its success or failure in different patients?
Research Title: The Impact of Climate Change on Biodiversity
- Research Question : How is climate change affecting global biodiversity, and what can be done to mitigate the negative effects on natural ecosystems?
Research Title: Exploring the Relationship between Cultural Diversity and Workplace Productivity
- Research Question : How does cultural diversity impact workplace productivity, and what strategies can be employed to maximize the benefits of a diverse workforce?
Research Title: The Role of Artificial Intelligence in Healthcare
- Research Question: How can artificial intelligence be leveraged to improve healthcare outcomes, and what are the potential risks and ethical concerns associated with its use?
Applications of Research Questions
Here are some of the key applications of research questions:
- Defining the scope of the study : Research questions help researchers to narrow down the scope of their study and identify the specific issues they want to investigate.
- Developing hypotheses: Research questions often lead to the development of hypotheses, which are testable predictions about the relationship between variables. Hypotheses provide a clear and focused direction for the study.
- Designing the study : Research questions guide the design of the study, including the selection of participants, the collection of data, and the analysis of results.
- Collecting data : Research questions inform the selection of appropriate methods for collecting data, such as surveys, interviews, or experiments.
- Analyzing data : Research questions guide the analysis of data, including the selection of appropriate statistical tests and the interpretation of results.
- Communicating results : Research questions help researchers to communicate the results of their study in a clear and concise manner. The research questions provide a framework for discussing the findings and drawing conclusions.
Characteristics of Research Questions
Characteristics of Research Questions are as follows:
- Clear and Specific : A good research question should be clear and specific. It should clearly state what the research is trying to investigate and what kind of data is required.
- Relevant : The research question should be relevant to the study and should address a current issue or problem in the field of research.
- Testable : The research question should be testable through empirical evidence. It should be possible to collect data to answer the research question.
- Concise : The research question should be concise and focused. It should not be too broad or too narrow.
- Feasible : The research question should be feasible to answer within the constraints of the research design, time frame, and available resources.
- Original : The research question should be original and should contribute to the existing knowledge in the field of research.
- Significant : The research question should have significance and importance to the field of research. It should have the potential to provide new insights and knowledge to the field.
- Ethical : The research question should be ethical and should not cause harm to any individuals or groups involved in the study.
Purpose of Research Questions
Research questions are the foundation of any research study as they guide the research process and provide a clear direction to the researcher. The purpose of research questions is to identify the scope and boundaries of the study, and to establish the goals and objectives of the research.
The main purpose of research questions is to help the researcher to focus on the specific area or problem that needs to be investigated. They enable the researcher to develop a research design, select the appropriate methods and tools for data collection and analysis, and to organize the results in a meaningful way.
Research questions also help to establish the relevance and significance of the study. They define the research problem, and determine the research methodology that will be used to address the problem. Research questions also help to determine the type of data that will be collected, and how it will be analyzed and interpreted.
Finally, research questions provide a framework for evaluating the results of the research. They help to establish the validity and reliability of the data, and provide a basis for drawing conclusions and making recommendations based on the findings of the study.
Advantages of Research Questions
There are several advantages of research questions in the research process, including:
- Focus : Research questions help to focus the research by providing a clear direction for the study. They define the specific area of investigation and provide a framework for the research design.
- Clarity : Research questions help to clarify the purpose and objectives of the study, which can make it easier for the researcher to communicate the research aims to others.
- Relevance : Research questions help to ensure that the study is relevant and meaningful. By asking relevant and important questions, the researcher can ensure that the study will contribute to the existing body of knowledge and address important issues.
- Consistency : Research questions help to ensure consistency in the research process by providing a framework for the development of the research design, data collection, and analysis.
- Measurability : Research questions help to ensure that the study is measurable by defining the specific variables and outcomes that will be measured.
- Replication : Research questions help to ensure that the study can be replicated by providing a clear and detailed description of the research aims, methods, and outcomes. This makes it easier for other researchers to replicate the study and verify the results.
Limitations of Research Questions
Limitations of Research Questions are as follows:
- Subjectivity : Research questions are often subjective and can be influenced by personal biases and perspectives of the researcher. This can lead to a limited understanding of the research problem and may affect the validity and reliability of the study.
- Inadequate scope : Research questions that are too narrow in scope may limit the breadth of the study, while questions that are too broad may make it difficult to focus on specific research objectives.
- Unanswerable questions : Some research questions may not be answerable due to the lack of available data or limitations in research methods. In such cases, the research question may need to be rephrased or modified to make it more answerable.
- Lack of clarity : Research questions that are poorly worded or ambiguous can lead to confusion and misinterpretation. This can result in incomplete or inaccurate data, which may compromise the validity of the study.
- Difficulty in measuring variables : Some research questions may involve variables that are difficult to measure or quantify, making it challenging to draw meaningful conclusions from the data.
- Lack of generalizability: Research questions that are too specific or limited in scope may not be generalizable to other contexts or populations. This can limit the applicability of the study’s findings and restrict its broader implications.
About the author

Muhammad Hassan
Researcher, Academic Writer, Web developer
You may also like

Ethical Considerations – Types, Examples and...

Appendix in Research Paper – Examples and...

Research Design – Types, Methods and Examples

Limitations in Research – Types, Examples and...

Context of the Study – Writing Guide and Examples

Delimitations in Research – Types, Examples and...
Literature Searching

Types of Research Questions
Research questions can be categorized into different types, depending on the type of research to be undertaken.
Qualitative questions concern broad areas or more specific areas of research and focus on discovering, explaining and exploring. Types of qualitative questions include:
- Exploratory Questions, which seeks to understand without influencing the results. The objective is to learn more about a topic without bias or preconceived notions.
- Predictive Questions, which seek to understand the intent or future outcome around a topic.
- Interpretive Questions, which tries to understand people’s behavior in a natural setting. The objective is to understand how a group makes sense of shared experiences with regards to various phenomena.
Quantitative questions prove or disprove a researcher’s hypothesis and are constructed to express the relationship between variables and whether this relationship is significant. Types of quantitative questions include:
- Descriptive questions , which are the most basic type of quantitative research question and seeks to explain the when, where, why or how something occurred.
- Comparative questions are helpful when studying groups with dependent variables where one variable is compared with another.
- Relationship-based questions try to answer whether or not one variable has an influence on another. These types of question are generally used in experimental research questions.
References/Additional Resources
Lipowski, E. E. (2008). Developing great research questions . American Journal of Health-System Pharmacy, 65(17), 1667–1670.
Ratan, S. K., Anand, T., & Ratan, J. (2019). Formulation of Research Question - Stepwise Approach . Journal of Indian Association of Pediatric Surgeons , 24 (1), 15–20.
Fandino W.(2019). Formulating a good research question: Pearls and pitfalls . I ndian J Anaesth. 63(8) :611-616.
Beck, L. L. (2023). The question: types of research questions and how to develop them . In Translational Surgery: Handbook for Designing and Conducting Clinical and Translational Research (pp. 111-120). Academic Press.
Doody, O., & Bailey, M. E. (2016). Setting a research question, aim and objective. Nurse Researcher, 23(4), 19–23.
Plano Clark, V., & Badiee, M. (2010). Research questions in mixed methods research . In: SAGE Handbook of Mixed Methods in Social & Behavioral Research . SAGE Publications, Inc.,
Agee, J. (2009). Developing qualitative research questions: A reflective process . International journal of qualitative studies in education , 22 (4), 431-447.
Flemming, K., & Noyes, J. (2021). Qualitative Evidence Synthesis: Where Are We at? I nternational Journal of Qualitative Methods, 20.
Research Question Frameworks
Research question frameworks have been designed to help structure research questions and clarify the main concepts. Not every question can fit perfectly into a framework, but using even just parts of a framework can help develop a well-defined research question. The framework to use depends on the type of question to be researched. There are over 25 research question frameworks available. The University of Maryland has a nice table listing out several of these research question frameworks, along with what the acronyms mean and what types of questions/disciplines that may be used for.
The process of developing a good research question involves taking your topic and breaking each aspect of it down into its component parts.
Booth, A., Noyes, J., Flemming, K., Moore, G., Tunçalp, Ö., & Shakibazadeh, E. (2019). Formulating questions to explore complex interventions within qualitative evidence synthesis. BMJ global health , 4 (Suppl 1), e001107. (See supplementary data#1)
The "Well-Built Clinical Question“: PICO(T)
One well-established framework that can be used both for refining questions and developing strategies is known as PICO(T). The PICO framework was designed primarily for questions that include interventions and comparisons, however other types of questions may also be able to follow its principles. If the PICO(T) framework does not precisely fit your question, using its principles (see alternative component suggestions) can help you to think about what you want to explore even if you do not end up with a true PICO question.
A PICO(T) question has the following components:
- P : The patient’s disorder or disease or problem of interest / research object
- I: The intervention, exposure or finding under review / Application of a theory or method
- C: A comparison intervention or control (if applicable- not always present)/ Alternative theories or methods (or, in their absence, the null hypothesis)
- O : The outcome(s) (desired or of interest) / Knowledge generation
- T : (The time factor or period)
Keep in mind that solely using a tool will not enable you to design a good question. What is required is for you to think, carefully, about exactly what you want to study and precisely what you mean by each of the things that you think you want to study.
Rzany, & Bigby, M. (n.d.). Formulating Well-Built Clinical Questions. In Evidence-based dermatology / (pp. 27–30). Blackwell Pub/BMJ Books.
Nishikawa-Pacher, A. (2022). Research questions with PICO: a universal mnemonic. Publications , 10 (3), 21.
- << Previous: Characteristics of a good research question
- Next: Choosing the Search Terms >>
- (855) 776-7763
Training Maker
All Products
Qualaroo Insights
ProProfs.com
- Get Started Free
FREE. All Features. FOREVER!
Try our Forever FREE account with all premium features!
How to Write Quantitative Research Questions: Types With Examples

Market Research Specialist
Emma David, a seasoned market research professional, specializes in employee engagement, survey administration, and data management. Her expertise in leveraging data for informed decisions has positively impacted several brands, enhancing their market position.

Has it ever happened that you conducted a quantitative research study and found out the results you were expecting are quite different from the actual results?
This could happen due to many factors like the unpredictable nature of respondents, errors in calculation, research bias, etc. However, your quantitative research usually does not provide reliable results when questions are not written correctly.
We get it! Structuring the quantitative research questions can be a difficult task.
Hence, in this blog, we will share a few bits of advice on how to write good quantitative research questions. We will also look at different types of quantitative research questions along with their examples.
Let’s start:
How to Write Quantitative Research Questions?
When you want to obtain actionable insight into the trends and patterns of the research topic to make sense of it, quantitative research questions are your best bet.
Being objective in nature, these questions provide you with detailed information about the research topic and help in collecting quantifiable data that can be easily analyzed. This data can be generalized to the entire population and help make data-driven and sound decisions.
Respondents find it easier to answer quantitative survey questions than qualitative questions. At the same time, researchers can also analyze them quickly using various statistical models.
However, when it comes to writing the quantitative research questions, one can get a little overwhelmed as the entire study depends on the types of questions used.
There is no “one good way” to prepare these questions. However, to design well-structured quantitative research questions, you can follow the 4-steps approach given below:
1. Select the Type of Quantitative Question
The first step is to determine which type of quantitative question you want to add to your study. There are three types of quantitative questions:
- Descriptive
- Comparative
- Relationship-based
This will help you choose the correct words and phrases while constructing the question. At the same time, it will also assist readers in understanding the question correctly.
2. Identify the Type of Variable
The second step involves identifying the type of variable you are trying to measure, manipulate, or control. Basically, there are two types of variables:
- Independent variable (a variable that is being manipulated)
- Dependent variable (outcome variable)

If you plan to use descriptive research questions, you have to deal with a number of dependent variables. However, where you plan to create comparative or relationship research questions, you will deal with both dependent and independent variables.
3. Select the Suitable Structure
The next step is determining the structure of the research question. It involves:
- Identifying the components of the question. It involves the type of dependent or independent variable and a group of interest (the group from which the researcher tries to conclude the population).
- The number of different components used. Like, as to how many variables and groups are being examined.
- Order in which these are presented. For example, the independent variable before the dependent variable or vice versa.
4. Draft the Complete Research Question
The last step involves identifying the problem or issue that you are trying to address in the form of complete quantitative survey questions . Also, make sure to build an exhaustive list of response options to make sure your respondents select the correct response. If you miss adding important answer options, then the ones chosen by respondents may not be entirely true.
Want to create a quantitative research survey hassle-free? Explore our library of 1,000,000+ readymade questions.
Types of Quantitative Research Questions With Examples
Quantitative research questions are generally used to answer the “who” and “what” of the research topic. For quantitative research to be effective, it is crucial that the respondents are able to answer your questions concisely and precisely. With that in mind, let’s look in greater detail at the three types of formats you can use when preparing quantitative market research questions.
1. Descriptive
Descriptive research questions are used to collect participants’ opinions about the variable that you want to quantify. It is the most effortless way to measure the particular variable (single or multiple variables) you are interested in on a large scale. Usually, descriptive research questions begin with “ how much,” “how often,” “what percentage,” “what proportion,” etc.
Examples of descriptive research questions include:
| Questions | Variable | Group |
|---|---|---|
| 1. How much rice do Indians consume per month? | Rice intake monthly | Indians |
| 2. How often do you use mobile apps for shopping purposes? | Mobile app used | a. Smartphone users |
| b. Shopping enthusiasts | ||
| 3. What is the preferred choice of cuisine for Americans? | Cuisine | Americans |
| 4. How often do students aged between 10-15 years use Instagram monthly? | Monthly use of Instagram | Students aged between 10-15 |
| 5. How often do middle-class adults go on vacation yearly? | Vacation | Middle-class adults |
2. Comparative
Comparative research questions help you identify the difference between two or more groups based on one or more variables. In general, a comparative research question is used to quantify one variable; however, you can use two or more variables depending on your market research objectives.
Comparative research questions examples include:
| Questions | Variable | Groups |
|---|---|---|
| 6. What is the difference in duration spent on social media between people aged 15- 20 and 20-25? | Time spent on social media | Group 1: People within the age group 15-20 |
| Group 2: People within the age group 20-25 | ||
| 7. What is the difference in the daily protein intake between men and women in America? | Daily protein intake | Group 1: Men based in America |
| Group 2: Women based in America | ||
| 8. What is the difference between watching web series weekly between a child and an adult? | Watching web series weekly | Group 1: Child |
| Group 2: Adult | ||
| 9. What is the difference in attitude towards sports between Millennial adults and older people born before 1981? | Attitude towards sports | Group 1: Millennial adults |
| Group 2: Older people born before 1981 | ||
| 10. What is the difference in the usage of Facebook between male and female American university students? | Usage of Facebook | Group 1: Male American university students |
| Group 2: Female American university students |
3. Relationship-based
Relationship research questions are used to identify trends, causal relationships, or associations between two or more variables. It is not vital to distinguish between causal relationships, trends, or associations while using these types of questions. These questions begin with “What is the relationship” between independent and dependent variables, amongst or between two or more groups.
Relationship-based quantitative questions examples include:
| Questions | Independent Variable | Dependent Variable | Group |
|---|---|---|---|
| 11. What is the relationship between gender and perspective towards comedy movies amongst Americans? | Perspective | Gender | Americans |
| 12. What is the relationship between job motivation and pay level amongst US residents? | Job motivation | Pay level | US residents |
| 13. What is the relationship between salary and shopping habits among the women of Australia? | Salary | Shopping habits | Australia |
| 14. What is the relationship between gender and fast food preference in young adults? | Gender | Fast food | Young Adults |
| 15. What is the relationship between a college degree and a job position in corporates? | College degree | Job Position | Corporates |
Ready to Write Your Quantitative Research Questions?
So, there you have it. It was all about quantitative research question types and their examples. By now, you must have figured out a way to write quantitative research questions for your survey to collect actionable customer feedback.
Now, the only thing you need is a good survey maker tool , like ProProfs Survey Maker , that will glide your process of designing and conducting your surveys . You also get access to various survey question types, both qualitative and quantitative, that you can add to any kind of survey along with professionally-designed survey templates .

About the author
Emma David is a seasoned market research professional with 8+ years of experience. Having kick-started her journey in research, she has developed rich expertise in employee engagement, survey creation and administration, and data management. Emma believes in the power of data to shape business performance positively. She continues to help brands and businesses make strategic decisions and improve their market standing through her understanding of research methodologies.
Related Posts

150+ Poll Questions to Engage Your Target Audience

Surveys vs Questionnaires: Compare the Differences

Close Ended Questions: A Complete Guide With Types & Examples

16 Advantages & Disadvantages of Questionnaires

How to Write Event Survey Questions: Guide With Examples & Best Practices
How to Create Online Questionnaire Easily
Root out friction in every digital experience, super-charge conversion rates, and optimize digital self-service
Uncover insights from any interaction, deliver AI-powered agent coaching, and reduce cost to serve
Increase revenue and loyalty with real-time insights and recommendations delivered to teams on the ground
Know how your people feel and empower managers to improve employee engagement, productivity, and retention
Take action in the moments that matter most along the employee journey and drive bottom line growth
Whatever they’re are saying, wherever they’re saying it, know exactly what’s going on with your people
Get faster, richer insights with qual and quant tools that make powerful market research available to everyone
Run concept tests, pricing studies, prototyping + more with fast, powerful studies designed by UX research experts
Track your brand performance 24/7 and act quickly to respond to opportunities and challenges in your market
Explore the platform powering Experience Management
- Free Account
- Product Demos
- For Digital
- For Customer Care
- For Human Resources
- For Researchers
- Financial Services
- All Industries
Popular Use Cases
- Customer Experience
- Employee Experience
- Net Promoter Score
- Voice of Customer
- Customer Success Hub
- Product Documentation
- Training & Certification
- XM Institute
- Popular Resources
- Customer Stories
- Artificial Intelligence
Market Research
- Partnerships
- Marketplace
The annual gathering of the experience leaders at the world’s iconic brands building breakthrough business results, live in Salt Lake City.
- English/AU & NZ
- Español/Europa
- Español/América Latina
- Português Brasileiro
- REQUEST DEMO
- Experience Management
- Qualitative Research Questions
Try Qualtrics for free
How to write qualitative research questions.
11 min read Here’s how to write effective qualitative research questions for your projects, and why getting it right matters so much.
What is qualitative research?
Qualitative research is a blanket term covering a wide range of research methods and theoretical framing approaches. The unifying factor in all these types of qualitative study is that they deal with data that cannot be counted. Typically this means things like people’s stories, feelings, opinions and emotions , and the meanings they ascribe to their experiences.
Qualitative study is one of two main categories of research, the other being quantitative research. Quantitative research deals with numerical data – that which can be counted and quantified, and which is mostly concerned with trends and patterns in large-scale datasets.
What are research questions?
Research questions are questions you are trying to answer with your research. To put it another way, your research question is the reason for your study, and the beginning point for your research design. There is normally only one research question per study, although if your project is very complex, you may have multiple research questions that are closely linked to one central question.
A good qualitative research question sums up your research objective. It’s a way of expressing the central question of your research, identifying your particular topic and the central issue you are examining.
Research questions are quite different from survey questions, questions used in focus groups or interview questions. A long list of questions is used in these types of study, as opposed to one central question. Additionally, interview or survey questions are asked of participants, whereas research questions are only for the researcher to maintain a clear understanding of the research design.
Research questions are used in both qualitative and quantitative research , although what makes a good research question might vary between the two.
In fact, the type of research questions you are asking can help you decide whether you need to take a quantitative or qualitative approach to your research project.
Discover the fundamentals of qualitative research
Quantitative vs. qualitative research questions
Writing research questions is very important in both qualitative and quantitative research, but the research questions that perform best in the two types of studies are quite different.
Quantitative research questions
Quantitative research questions usually relate to quantities, similarities and differences.
It might reflect the researchers’ interest in determining whether relationships between variables exist, and if so whether they are statistically significant. Or it may focus on establishing differences between things through comparison, and using statistical analysis to determine whether those differences are meaningful or due to chance.
- How much? This kind of research question is one of the simplest. It focuses on quantifying something. For example:
How many Yoruba speakers are there in the state of Maine?
- What is the connection?
This type of quantitative research question examines how one variable affects another.
For example:
How does a low level of sunlight affect the mood scores (1-10) of Antarctic explorers during winter?
- What is the difference? Quantitative research questions in this category identify two categories and measure the difference between them using numerical data.
Do white cats stay cooler than tabby cats in hot weather?
If your research question fits into one of the above categories, you’re probably going to be doing a quantitative study.
Qualitative research questions
Qualitative research questions focus on exploring phenomena, meanings and experiences.
Unlike quantitative research, qualitative research isn’t about finding causal relationships between variables. So although qualitative research questions might touch on topics that involve one variable influencing another, or looking at the difference between things, finding and quantifying those relationships isn’t the primary objective.
In fact, you as a qualitative researcher might end up studying a very similar topic to your colleague who is doing a quantitative study, but your areas of focus will be quite different. Your research methods will also be different – they might include focus groups, ethnography studies, and other kinds of qualitative study.
A few example qualitative research questions:
- What is it like being an Antarctic explorer during winter?
- What are the experiences of Yoruba speakers in the USA?
- How do white cat owners describe their pets?
Qualitative research question types
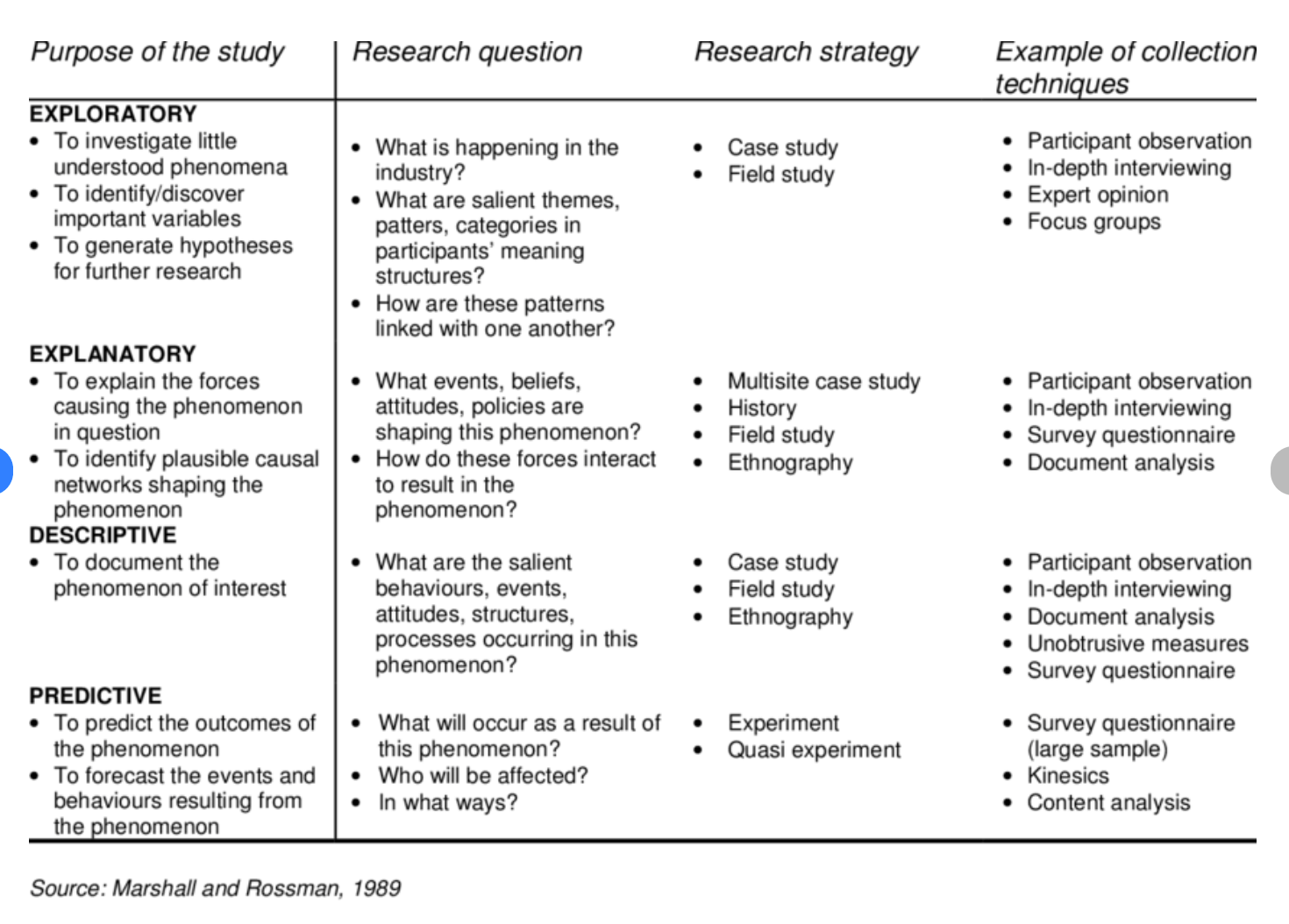
Marshall and Rossman (1989) identified 4 qualitative research question types, each with its own typical research strategy and methods.
- Exploratory questions
Exploratory questions are used when relatively little is known about the research topic. The process researchers follow when pursuing exploratory questions might involve interviewing participants, holding focus groups, or diving deep with a case study.
- Explanatory questions
With explanatory questions, the research topic is approached with a view to understanding the causes that lie behind phenomena. However, unlike a quantitative project, the focus of explanatory questions is on qualitative analysis of multiple interconnected factors that have influenced a particular group or area, rather than a provable causal link between dependent and independent variables.
- Descriptive questions
As the name suggests, descriptive questions aim to document and record what is happening. In answering descriptive questions , researchers might interact directly with participants with surveys or interviews, as well as using observational studies and ethnography studies that collect data on how participants interact with their wider environment.
- Predictive questions
Predictive questions start from the phenomena of interest and investigate what ramifications it might have in the future. Answering predictive questions may involve looking back as well as forward, with content analysis, questionnaires and studies of non-verbal communication (kinesics).
Why are good qualitative research questions important?
We know research questions are very important. But what makes them so essential? (And is that question a qualitative or quantitative one?)
Getting your qualitative research questions right has a number of benefits.
- It defines your qualitative research project Qualitative research questions definitively nail down the research population, the thing you’re examining, and what the nature of your answer will be.This means you can explain your research project to other people both inside and outside your business or organization. That could be critical when it comes to securing funding for your project, recruiting participants and members of your research team, and ultimately for publishing your results. It can also help you assess right the ethical considerations for your population of study.
- It maintains focus Good qualitative research questions help researchers to stick to the area of focus as they carry out their research. Keeping the research question in mind will help them steer away from tangents during their research or while they are carrying out qualitative research interviews. This holds true whatever the qualitative methods are, whether it’s a focus group, survey, thematic analysis or other type of inquiry.That doesn’t mean the research project can’t morph and change during its execution – sometimes this is acceptable and even welcome – but having a research question helps demarcate the starting point for the research. It can be referred back to if the scope and focus of the project does change.
- It helps make sure your outcomes are achievable
Because qualitative research questions help determine the kind of results you’re going to get, it helps make sure those results are achievable. By formulating good qualitative research questions in advance, you can make sure the things you want to know and the way you’re going to investigate them are grounded in practical reality. Otherwise, you may be at risk of taking on a research project that can’t be satisfactorily completed.
Developing good qualitative research questions
All researchers use research questions to define their parameters, keep their study on track and maintain focus on the research topic. This is especially important with qualitative questions, where there may be exploratory or inductive methods in use that introduce researchers to new and interesting areas of inquiry. Here are some tips for writing good qualitative research questions.
1. Keep it specific
Broader research questions are difficult to act on. They may also be open to interpretation, or leave some parameters undefined.
Strong example: How do Baby Boomers in the USA feel about their gender identity?
Weak example: Do people feel different about gender now?
2. Be original
Look for research questions that haven’t been widely addressed by others already.
Strong example: What are the effects of video calling on women’s experiences of work?
Weak example: Are women given less respect than men at work?
3. Make it research-worthy
Don’t ask a question that can be answered with a ‘yes’ or ‘no’, or with a quick Google search.
Strong example: What do people like and dislike about living in a highly multi-lingual country?
Weak example: What languages are spoken in India?
4. Focus your question
Don’t roll multiple topics or questions into one. Qualitative data may involve multiple topics, but your qualitative questions should be focused.
Strong example: What is the experience of disabled children and their families when using social services?
Weak example: How can we improve social services for children affected by poverty and disability?
4. Focus on your own discipline, not someone else’s
Avoid asking questions that are for the politicians, police or others to address.
Strong example: What does it feel like to be the victim of a hate crime?
Weak example: How can hate crimes be prevented?
5. Ask something researchable
Big questions, questions about hypothetical events or questions that would require vastly more resources than you have access to are not useful starting points for qualitative studies. Qualitative words or subjective ideas that lack definition are also not helpful.
Strong example: How do perceptions of physical beauty vary between today’s youth and their parents’ generation?
Weak example: Which country has the most beautiful people in it?
Related resources
Qualitative research design 12 min read, primary vs secondary research 14 min read, business research methods 12 min read, qualitative research interviews 11 min read, market intelligence 10 min read, marketing insights 11 min read, ethnographic research 11 min read, request demo.
Ready to learn more about Qualtrics?
Transforming the understanding and treatment of mental illnesses.
Información en español
Celebrating 75 Years! Learn More >>
- Science News
- Meetings and Events
- Social Media
- Press Resources
- Email Updates
- Innovation Speaker Series
Day Two: Placebo Workshop: Translational Research Domains and Key Questions
July 11, 2024
July 12, 2024
Day 1 Recap and Day 2 Overview
ERIN KING: All right. It is 12:01 so we'll go ahead and get started. And so on behalf of the Co-Chairs and the NIMH Planning Committee, I'd like to welcome you back to day two of the NIMH Placebo Workshop, Translational Research Domains and Key Questions. Before we begin, I will just go over our housekeeping items again. So attendees have been entered into the workshop in listen-only mode with cameras disabled. You can submit your questions via the Q&A box at any time during the presentation. And be sure to address your question to the speaker that you would like to respond.
For more information on today's speakers, their biographies can be found on the event registration website. If you have technical difficulties hearing or viewing the workshop, please note these in the Q&A box and our technicians will work to fix the problem. And you can also send an e-mail to [email protected]. And we'll put that e-mail address in the chat box for you. This workshop will be recorded and posted to the NIMH event web page for later viewing.
Now I would like to turn it over to our workshop Co-Chair, Dr. Cristina Cusin, for today's introduction.
CRISTINA CUSIN: Thank you so much, Erin. Welcome, everybody. It's very exciting to be here for this event.
My job is to provide you a brief recap of day one and to introduce you to the speakers of day two. Let me share my slides.
Again, thank you to the amazing Planning Committee. Thanks to their effort, we think this is going to be a success. I learned a lot of new information and a lot of ideas for research proposals and research projects from day one. Very briefly, please go and watch the videos. They are going to be uploaded in a couple of weeks if you missed them.
But we had an introduction from Tor, my Co-Chair. We had an historic perspective on clinical trials from the industry regulatory perspective. We had the current state from the FDA on placebo.
We had an overview of how hard it is to sham, to provide the right sham for device-based trials, and the challenges for TMS. We have seen some new data on the current state of placebo in psychosocial trials and what is the equivalent of a placebo pill for psychosocial trials. And some social neuroscience approach to placebo analgesia. We have come a long way from snake oil and we are trying to figure out what is placebo.
Tor, my Co-Chair, presented some data on the neurocircuitry underlying placebo effect and the questions that how placebo is a mixture of different elements including regression to the mean, sampling bias, selective attrition for human studies, the natural history of illness, the placebo effect per se that can be related to expectations, context, learning, interpretation.
We have seen a little bit of how is the impact on clinical trial design and how do we know that something, it really works. Or whatever this "it" is. And why do even placebo effect exists? It's fascinating idea that placebo exists as a predictive control to anticipate threats and the opportunity to respond in advance and to provide causal inference, a construct perception to infer the underlying state of body and of world.
We have seen historical perspective. And Ni Aye Khin and Mike Detke provided some overview of 25 years of randomized control trials from the data mining in major depressive disorders, schizophrenia trials and the lessons we have learned.
We have seen some strategies, both historical strategies and novel strategies to decrease placebo response in clinical trials and the results. Start from trial design, SPCD, lead-in, placebo phase and flexible dosing. Use of different scales. The use of statistical approaches like last observation carried forward or MMRM. Centralized ratings, self-rating, computer rating for different assessments. And more issues in clinical trials related to patient selection and professional patients.
Last, but not least, the dream of finding biomarkers for psychiatric conditions and tying response, clinical response to biomarkers. And we have seen how difficult it is to compare more recent studies with studies that were started in the '90s.
We have the FDA perspective with Tiffany Farchione in this placebo being a huge issue from the FDA. Especially the discussion towards the end of the day was on how to blind psychedelics.
We have seen an increasing placebo response rate in randomized controlled trials, also in adolescents, that is. And the considerations from the FDA of novel design models in collaboration with industry. We had examples of drugs approved for other disorders, not psychiatric condition, and realized -- made me realize how little we know about the true pathophysiology of psychiatric disorders, likely also heterogeneous conditions.
It made me very jealous of other fields because they have objective measures. They have biology, they have histology, they have imaging, they have lab values. While we are -- we are far behind, and we are not really able to explain to our patients why our mitigations are supposed to work or how they really work.
We heard from Holly Lisanby and Zhi-De Deng. The sham, the difficulty in producing the right sham for each type of device because most of them have auxiliary effects that are separate from the clinical effect like the noise or the scalp stimulation for TMS.
And it's critical to obtain a true blinding and separating sham from verum. We have seen how in clinical trials for devices expectancy from the patient, high tech environment and prolonged contact with clinicians and staff may play a role. And we have seen how difficult it is to develop the best possible sham for TMS studies in tDCS. It's really complicated and it's so difficult also to compare published studies in meta-analysis because they've used very different type of sham. Not all sham are created equal. And some of them could have been biologically active, so therefore invalidating the result or making the study uninformative.
Then we moved on to another fascinating topic with Dr. Rief and Dr. Atlas. What is the impact of psychological factors when you're studying a psychological intervention. Expectations, specific or nonspecific factors in clinical trials and what is interaction between those factors.
More, we learned about the potential nocebo effect of standard medical care or being on a wait list versus being in the active arm of a psychotherapy trial. And the fact that we are not accurately measuring the side effect of psychotherapy trial itself. And we heard more a fascinating talk about the neurocircuitry mediating placebo effect -- salience, affective value, cognitive control. And how perception of provider, perception of his or her warmth and competence and other social factors can affect response and placebo response, induce bias in evaluation of acute pain of others. Another very interesting field of study.
From a clinician perspective, this is -- and from someone who conduct clinical trials, all this was extremely informative because in many case in our patient situation no matter how good the treatment is, they have severe psychosocial stressors. They have difficulties to accessing food, to access treatment, transportation, or they live in an extremely stressful environment. So to disentangle other psychosocial factors from the treatment, from the biology is going to be critical to figure out how to treat best our patients.
And there is so much more work to do. Each of us approach the placebo topic for research from a different perspective. And like the blind man trying to understand what is an elephant, we have to endure it, we have to talk to each other, we have to collaborate and understand better the underlying biology, understand different aspect of the placebo phenomena.
And this lead us to the overview for day two. We are going to hear more about other topic that are so exciting. The placebo, the nocebo effect and other predictive factors in laboratory setting. We are going to hear about genetic of the placebo response to clinical trials. More physiological and psychological and neuromechanism for analgesia. And after a brief break around 1:30, we are going to hear about novel biological and behavioral approaches for the placebo effect.
We are going to hear about brain mapping. We are going to hear about other findings from imaging. And we're going to hear about preclinical modeling. There were some questions yesterday about animal models of placebo. And last, but not least, please stay around because in the panel discussion, we are going to tackle some of your questions. And we are going to have two wonderful moderators, Ted Kaptchuk and Matthew Rudorfer. So please stay with us and ask questions. We love to see more challenges for our speakers. And we're going to be all of the panelists from yesterday, from today are going to be present. Thank you so much.
Now we're going to move on to our first speaker of the day. If I am correct according to the last -- Luana.
Measuring & Mitigating the Placebo Effect
LUANA COLLOCA: Thank you very much, Cristina. First, I would love to thank the organizer. This is a very exciting opportunity to place our awareness about this important phenomenon for clinical trials and the clinical practice.
And today, I wish to give you a very brief overview of the psychoneurobiological mechanism of a placebo and nocebo, the description of some pharmacological studies, and a little bit of information on social learning. That is a topic that has been mentioned a little bit yesterday. And finally, the translational part. Can we translate what we learn from mechanistic approach to placebo and nocebo in terms of a disease and symptomatology and eventually predictors is the bigger question.
So we learned yesterday that placebo effects are generated by verbal suggestion, this medication has strong antidepressant effects. Therapeutic prior experience, merely taking a medication weeks, days before being substitute with a simulation of placebo sham treatment. Observation of a benefit in other people, contextual and treatment cue, and interpersonal interactions.
Especially in the fields of pain where we can simulate nociception, painful experience in laboratory setting, we learn a lot about the modulation related to placebo. In particular, expectation can provide a reaction and activation of parts of the brain like frontal area, nucleus accumbens, ventral striatum. And this kind of mechanism can generate a descending stimulation to make the painful nociceptive stimulus less intense.
The experience of analgesia at the level of a pain mechanism translate into a modulation reduction of a pain intensity. But most important, pain unpleasantness and the effective components of the pain. I will show today some information about the psychological factor, the demographic factor as well as genetic factors that can be predictive of placebo effects in the context of a pain.
On the other hand, a growing interest is related to nocebo effects, the negative counter sides of this phenomenon. When we talk about nocebo effects, we refer to increase in worsening of outcome in symptoms related to negative expectation, prior negative therapeutic experience, observing a negative outcome in others, or even mass psychogenic modeling such as some nocebo-related response during the pandemic. Treatment leaflets, the description of all side effects related to a medication. Patient-clinician communication. The informed consent where we list all of the side effects of a procedure or medication as well as contextual cues in clinical encounters.
And importantly, internal factor like emotion, mood, maladaptive cognitive appraisal, negative valence, personality traits, somatosensory features and omics can be predictive of negative worsening of symptom and outcome related to placebo and nocebo effects. In terms of a nocebo very briefly, there is a lot of attention again related to brain imaging with beautiful data show that the brainstem, the spinal cord, the hippocampus play a critical role during nocebo hyperalgesic effects.
And importantly, we learn that about placebo and nocebo through different approach including brain imaging, as we saw yesterday, but also pharmacological approach. We start from realizing that placebo effects are really neurobiological effects with the use of agonist or antagonist.
In other words, we can use a drug to mimic the action of that drug when we replace the drug with a saline solution, for example. In the cartoon here, you can see a brief pharmacological conditioning with apomorphine. Apomorphine is a dopamine agonist. And after three days of administration, apomorphine was replaced with saline solution in the intraoperative room to allow us to understand if we can mimic at the level of neuronal response the effects of apomorphine.
So in brief these are patients undergoing subthalamic EEG installation of deep brain stimulation. You can see here reaching the subthalamic nucleus. So after crossing the thalamus, the zona incerta, the STN, and the substantia nigra, the surgeon localized the area of stimulation. Because we have two subthalamic nuclei, we can use one as control and the other one as target to study in this case the effects of saline solution given after three days of apomorphine.
What we found was in those people who respond, there was consistency in reduction of clinical symptoms. As you can see here, the UPDRS, a common scale to measure rigidity in Parkinson, the frequency of a discharge at the level of neurons and the self-perception, patients with sentences like I feel like after Levodopa, I feel good. This feeling good translate in less rigidity, less tremor in the surgical room.
On the other hand, some participants didn't respond. Consistently we found no clinical improvement, no difference in preference over this drug at the level of a single unit and no set perception of a benefit. This kind of effects started to trigger the questions what is the reason why some people who responded to placebo and pharmacological conditioning and some other people don't. I will try to address this question in the second part of my talk.
On the other hand, we learn a lot about the endogenous modulation of pain and true placebo effects by using in this case an antagonist. The goal in this experiment was to create a painful sensation through a tourniquet. Week one with no treatment. Week two we pre-inject healthy participant with morphine. Week three the same morphine. And week four we replace morphine with placebo.
And you can see that a placebo increase the pain tolerance in terms of imminent. And this was not carryover effects. In fact, the control at week five showed no differences. Part of the participants were pre-injected with an antagonist Naloxone that when we use Naloxone at high dose, we can block the opioids delta and K receptors. You can see that by pre-injecting Naloxone there is a blockage of placebo analgesia, and I would say this morphine-like effects related to placebo given after morphine.
We start to then consider this phenomenon. Is this a way for tapering opioids. And we called this sort of drug-like effects as dose-extending placebo. The idea is that if we use a pharmacological treatment, morphine, apomorphine, as I showed to you, and then we replace the treatment with a placebo, we can create a pharmacological memory, and this can translate into a clinical benefit. Therefore, the dose-extending placebo can be used to extend the benefit of the drug, but also to reduce side effects related to the active drug.
In particular for placebo given after morphine, you can see on this graph, the effects is similarly strong if we do the repetition of a morphine one day apart or one week apart. Interestingly, this is the best model to be used in animal research.
Here at University of Maryland in collaboration with Todd Degotte, we create a model of anhedonia in mice and we condition animals with Ketamine. The goal was to replace Ketamine with a placebo. There are several control as you can see. But what is important for us, we condition animal with Ketamine week one, three and five. And then we substitute Ketamine with saline along with the CS. The condition of the stimulus was a light, a low light. And we want to compare this with an injection of Ketamine given at week seven.
So as you can see here, of course Ketamine was inducing a benefit as compared to saline and the Ketamine. But what is seen testing when we compare Ketamine week seven with saline replacing the Ketamine, we found no difference; suggesting that even in animals, in mice we were able to create drug-related effects. In this case, a Ketamine antidepressant-like placebo effects. These effects also add dimorphic effects in the sense that we observed this is in males but not in females.
So another approach to use agonist, like I mentioned for apomorphine in Parkinson patient, was to use vasopressin and oxytocin to increase placebo effects. In this case, we used verbal suggestion that in our experience especially with healthy participants tended to create very small sample size in terms of placebo analgesic effects. So we knew that from the literature that there is a dimorphic effects for this hormone. So we inject people with intranasal vasopressin, saline, oxytocin in low dose and no treatment. You can see there was a drug effects in women whereby vasopressin boost placebo analgesic effects, but not in men where yet we found many effects of manipulation but not drug effects.
Importantly, vasopressin affect dispositional anxiety as well as cortisol. And there is a negative correlation between anxiety and cortisol in relationship to vasopressin-induced placebo analgesia.
Another was, can we use medication to study placebo in laboratory setting or can we study placebo and nocebo without any medication? One example is to use a manipulation of the intensity of the painful stimulations. We use a thermal stimulation tailored at three different levels. 80 out of 100 with a visual analog scale, 50 or 20, as you can see from the thermometer.
We also combined the level of pain with a face. So first to emphasize there is three level of pain, participants will see an anticipatory cue just before the thermal stimulation. Ten seconds of the thermal stimulation to provide the experience of analgesia with the green and the hyperalgesia with the red as compared to the control, the yellow condition.
Therefore, the next day we move in the fMRI. And the goal was to try to understand to what extent expectation is relevant in placebo and nocebo effects. We mismatch what they anticipate, and they learn the day before. But also you can see we tailored the intensity at the same identical level. 50 for each participant.
We found that when expectation matched the level of the cues, anticipatory cue and face, we found a strong nocebo effects and placebo effects. You can see in red that despite the level of pain were identical, the perceived red-related stimuli as higher in terms of intensity, and the green related the stimuli as lower when compared to the control. By mismatching what they expect with what they saw, we blocked completely placebo effects and still nocebo persist.
So then I showed to you that we can use conditioning in animals and in humans to create placebo effects. But also by suggestion, the example of vasopressin. Another important model to study placebo effects in laboratory setting is social observation. We see something in other people, we are not told what we are seeing and we don't experience the thermal stimulation. That is the setting. A demonstrator receiving painful or no painful stimulation and someone observing this stimulation.
When we tested the observers, you can see the level of pain were tailored at the same identical intensity. And these were the effects. In 2009, when we first launched this line of research, this was quite surprising. We didn't anticipate that merely observing someone else could boost the expectations and probably creating this long-lasting analgesic effect. This drove our attention to the brain mechanism of what is so important during this transfer of placebo analgesia.
So we scanned participants when they were observing a video this time. And a demonstrator receiving control and placebo cream. We counterbalance the color. We controlled for many variables. So during the observation of another person when they were not stimulated, they didn't receive the cream, there is an activation of the left and right temporoparietal junction and a different activation of the amygdala with the two creams. And importantly, an activation of the periaqueductal gray that I show to you is critical in modulating placebo analgesia.
Afterwards we put both the placebo creams with the two different color. We tailored the level of pain at the identical level of intensity. And we saw how placebo effects through observation are generated. They create strong different expectation and anxiety. And importantly, we found that the functional connectivity between the dorsolateral prefrontal cortex and temporoparietal junction that was active during the observation mediate the behavior results. Suggesting that there is some mechanism here that may be relevant to exploit in clinical trials and clinical practice.
From this, I wish to switch to a more translational approach. Can we replicate these results observed in health participant for nociception in people suffering from chronic pain. So we chose as population of facial pain that is an orphan disease that has no consensus on how to treat it, but also it affects the youngest including children.
So participants were coming to the lab. And thus you can see we used the same identical thermal stimulation, the same electrodes, the same conditioning that I showed to you. We measured expectation before and after the manipulation. The very first question was can we achieve similar monitored distribution of placebo analgesia in people suffering chronically from pain and comorbidities. You can see that we found no difference between temporo parenthala, between TMD and controls. Also, we observed that some people responded to the placebo manipulation with hyperalgesia. We call this nocebo effect.
Importantly, these affects are less relevant than the benefit that sometime can be extremely strong show that both health control and TMD. Because we run experiment in a very beautiful ecological environment where we are diverse, the lab, the experimenters as well as the population we recruit in the lab has a very good distribution of race, ethnicity.
So the very first question was we need to control for this factor. And this turned out to be a beautiful model to study race, ethnicity in the lab. So when chronic pain patient were studied by same experimenter race, dark blue, we observe a larger placebo effect. And this tell us about the disparity in medicine. In fact, we didn't see these effects in our controls.
In chronic pain patient, we also saw a sex concordance influence. But in the opposite sense in women studied by a man experimenter placebo effects are larger. Such an effect was not seen in men.
The other question that we had was what about the contribution of psychological factors. At that stage, there were many different survey used by different labs. Some are based on the different area of, you know, the states of the world, there were trends where in some people in some study they observe an effects of neurodisease, more positive and negative set, that refer to the words. Instead of progressing on single survey, and now we have a beautiful meta-analysis today that is not worth in the sense that it is not predictive of placebo effects.
We use the rogue model suggested by the NIMH. And by doing a sophisticated approach we were able to combine this into four balances. Emotional distress, reward-seeking, pain related fear catastrophizing, empathy and openness. These four valences then were interrelated to predict placebo effects. And you can see that emotional distress is associated with lower magnitude of placebo effects extinguishing over time and lower proportion of placebo responsivity.
Also people who tend to catastrophizing display lower magnitude of placebo effects. In terms of expectation, it is also interesting patients expect to benefit, they have this desire for a reward. But also those people who are more open and characterized by empathy tend for the larger expectations. But this doesn't translate necessarily in larger placebo effects, somehow hinting that the two phenomenon can be not necessarily linked.
Because we study chronic pain patients they come with their own baggage of disease comorbidities. And Dr. Wang in his department look at insomnia. Those people suffering from insomnia tends to have lower placebo analgesic effects along with those who have a poor pattern of sleep, suggesting that clinical factor can be relevant when we wish to predict placebo effects.
Another question that we address how simple SNPs, single nucleotide polymorphism variants in three regions that have been published can be predictive of placebo effects. In particular, I'm referring to OPRM1 that is linked to the gene for endogenous opioids. COMT linked to endogenous dopamine. And FAAH linked to endogenous cannabinoids. And we will learn about that more with the next talk.
And you can see that there is a prediction. These are rogue codes that can be interesting. We model all participants with verbal suggestion alone, the conditioning. There isn't really a huge difference between using one SNP versus two or three. What is truly impact and was stronger in terms of prediction was accounting for the procedure we used to study placebo. Whether by suggestion alone versus condition. When we added the manipulation, the prediction becomes stronger.
More recently, we started gene expression transcriptomic profile associated with placebo effects. We select from the 402 participants randomly 54. And we extract their transcriptomic profiles. Also we select a validation cohort to see if we can't replicate what we discover in terms of mRNA sequencing. But we found over 600 genes associated with the discovered cohort. In blue are the genes downregulated and in red upregulated.
We chose the top 20 genes and did the PCA to validate the top 20. And we found that six of them were replicated and they include all these genes that you see here. The Selenom for us was particularly interesting, as well as the PI3, the CCDC85B, FBXL15, HAGHL and the TNFRSF4. So with this --
LUANA COLLOCA: Yes, I'm done. With this, that is the goal probably one day with AI and other approach to combine clinical psychological brain imaging and so on, characteristic and behavior to predict a level of transitory response to placebo. That may guide us in clinical trials and clinical path to tailor the treatment. Therefore, the placebo and nocebo biological response can be to some extent predicted. And identify those who responded to placebo can help tailoring drug development and symptom management.
Thank you to my lab. All of you, the funding agencies. And finally, for those who like to read more about placebo, this book is available for free to be downloaded. And they include many of the speakers from this two-day event as contributors to this book. Thank you very much.
CRISTINA CUSIN: Thank you so much, Luana. It was a wonderful presentation. We have one question in the Q&A.
Elegant studies demonstrating powerful phenomena. Two questions. Is it possible to extend or sustain placebo-boosting effect? And what is the dose response relationship with placebo or nocebo?
LUANA COLLOCA: Great questions. The goal is to boost a placebo effects. And one way, as I showed was, for example, using intranasal vasopressin. But also extending relationship with placebo we know that we need the minimum of a three or four other administration before boosting this sort of pharmacological memory. And the longer is the administration of the active drug before we replace with placebo, the larger the placebo effects.
For nocebo, we show similar relationship with the collaborators. So again, the longer we condition, the stronger the placebo or nocebo effects. Thank you so much.
CRISTINA CUSIN: I wanted to ask, do you have any theory or interpretation about the potential for transmit to person a placebo response between the observer or such, do you have any interpretation of this phenomenon?
LUANA COLLOCA: It is not completely new in the literature. There is a lot of studies show that we can transfer pain in both animal models and humans.
So transfer analgesia is a natural continuation of that line of research. And the fact that we mimic things that we see in some other people, this is the very most basic form of learning when we grow up. But also from a revolutionary point of view protect us from predators and animals and us as human beings observing is a very good mechanism to boost behaviors and in this case placebo effects. Thank you.
CRISTINA CUSIN: Okay. We will have more time to ask questions.
We are going to move on to the next speaker. Dr. Kathryn Hall.
KATHRYN HALL: Thank you. Can you see my screen okay? Great.
So I'm going to build on Dr. Colloca's talk to really kind of give us a deeper dive into the genetics of the placebo response in clinical trials.
So I have no disclosures. So as we heard and as we have been hearing over the last two days, there is -- there are physiological drivers of placebo effects, whether they are opioid signaling or dopamine signaling. And these are potentiated by the administration or can be potentiated by saline pills, saline injections, sugar pills. And what's really interesting here, I think, is this discussion about how drugs impact the drivers of placebo response. In particular we heard about Naloxone yesterday and proglumide.
What I really want to do today is think about the next layer. Like how do the genes that shape our biology and really drive or influence that -- those physiological drivers of placebo response, how do the genes, A, modify our placebo response? But also, how are they modifying the effect of the drugs and the placebos on this basic -- this network?
And if you think about it, we really don't know much about all of the many interactions that are happening here. And I would actually argue that it goes even beyond genetic variation to other factors that lead to heterogeneity in clinical trials. Today I'm going to really focus on genes and variations in the genome.
So let's go back so we have the same terminology. I'm going to be talking about placebo-responsing trials. And so we saw this graph or a version of this graph yesterday where in clinical trials when we want to assess the effect of a drug, we subtract the outcomes in the placebo arm from the outcomes in the drug treatment arm. And there is a basic assumption here that the placebo response is additive to the drug response.
And what I want to do today is to really challenge that assumption. I want to challenge that expectation. Because I think we have enough literature and enough studies that have already been done that demonstrate that things are not as simple as that and that we might be missing a lot from this basic averaging and subtracting that we are doing.
So the placebo response is that -- is the bold lines there which includes placebo effects which we have been focusing on here. But it also includes a natural history of the disease or the condition, phenomenon such as statistical regression not mean, blinding and bias and Hawthorn effects. So we lump all of those together in the placebo arm of the trial and subtract the placebo response from the drug response to really understand the drug effect.
So one way to ask about, well, how do genes affect this is to look at candidate genes. And as Dr. Colloca pointed out and has done some very elegant studies in this area, genes like COMT, opioid receptors, genes like OPRM1, the FAAH endocannabinoid signaling genes are all candidate genes that we can look at in clinical trials and ask did these genes modify what we see in the placebo arm of trials?
We did some studies in COMT. And I want to just show you those to get a -- so you can get a sense of how genes can influence placebo outcomes. So COMT is catacholamethyl transferase. And it's a protein, an enzyme that metabolizes dopamine which as you saw is important in mediating the placebo response. COMT also metabolizes epinephrin, norepinephrine and catecholest estrogen. So the fact that COMT might be involved in placebo response is really interesting because it might be doing more than just metabolizing dopamine.
So we asked the question what happens if we look at COMT genetic variation in clinical trials of irritable bowel syndrome? And working with Ted Kaptchuk and Tony Lembo at Beth Israel Deaconess Medical Center, we did just that. We looked at COMT effects in a randomized clinical trial of irritable bowel syndrome. And what we did see was that for the gene polymorphism RS46AD we saw that people who had the weak version of the COMT enzyme actually had more placebo response. These are the met/met people here shown on this, in this -- by this arrow. And that the people who had less dopamine because that enzyme didn't work as well for this polymorphism, they had less of a placebo response in one of the treatment arms. And we would later replicate this study in another clinical trial that was recently concluded in 2021.
So to get a sense, as you can see, we are somewhat -- we started off being somewhat limited by what was available in the literature. And so we wanted to expand on that to say more about genes that might be associated with placebo response. So we went back, and we found 48 studies in the literature where there was a gene that was looked at that modified the placebo response.
And when we mapped those to the interactome, which is this constellation of all gene products and their interactions, their physical interactions, we saw that the placebome or the placebo module had certain very interesting characteristics. Two of those characteristics that I think are relevant here today are that they overlapped with the targets of drugs, whether they were analgesics, antidepressive drugs, anti-Parkinson's agents, placebo genes putatively overlapped with drug treatment genes or targets.
They also overlapped with disease-related genes. And so what that suggests is that when we were looking at the outcomes of clinical trial there might be a lot more going on that we are missing.
And let's just think about that for a minute. On the left is what we expect. We expect that we are going to see an effect in the drug, it's going to be greater than the effect of the placebo and that difference is what we want, that drug effect. But what we often see is on the right here where there is really no difference between drug and placebo. And so we are left to scratch our heads. Many companies go out of business. Many sections of companies close. And, quite frankly, patients are left in need. Money is left on the table because we can't discern between drug and placebo.
And I think what is interesting is that's been a theme that's kind of arisen since yesterday where oh, if only we had better physiological markers or better genes that targeted physiology then maybe we could see a difference and we can, you know, move forward with our clinical trials.
But what I'm going to argue today is actually what we need to do is to think about what is happening in the placebo arm, what is contributing to the heterogeneity in the placebo arm, and I'm going to argue that when we start to look at that compared to what is happening in the drug treatment arm, oftentimes -- and I'm going to give you demonstration after demonstration. And believe me, this is just the tip of the iceberg.
What we are seeing is there are differential effects by genotype in the drug treatment arm and the placebo treatment arm such that if you average out what's happening in these -- in these drug and placebo arms, you would basically see that there is no difference. But actually there's some people that are benefiting from the drug but not placebo. And conversely, benefiting from placebo but not drug. Average out to no difference.
Let me give you some examples. We had this hypothesis and we started to look around to see if we could get partners who had already done clinical trials that had happened to have genotyped COMT. And what we saw in this clinical trial for chronic fatigue syndrome where adolescents were treated with clonidine was that when we looked in the placebo arm, we saw that the val/val patients, so this is the COMT genotype. The low activity -- sorry, that is high activity genotype. They had the largest number increase in the number of steps they were taking per week. In contrast, the met/met people, the people with the weaker COMT had fewer, almost no change in the number of steps they were taking per week.
So you would look at this and you would say, oh, the val/val people were the placebo responders and the met/met people didn't respond to placebo. But what we saw when we looked into the drug treatment arm was very surprising. We saw that clonidine literally erased the effect that we were seeing in placebo for the val/val participants in this trial. And clonidine basically was having no effect on the heterozygotes, the val/mets or on the met/mets. And so this trial rightly concluded that there was no benefit for clonidine.
But if they hadn't taken this deeper look at what was happening, they would have missed that clonidine may potentially be harmful to people with chronic fatigue in this particular situation. What we really need to do I think is look not just in the placebo or not just in the drug treatment arm but in both arms to understand what is happening there.
And I'm going to give you another example. And, like I said, the literature is replete with these examples. On the left is an example from a drug that was used to test cognitive -- in cognitive scales, Tolcupone, which actually targets COMT. And what you can see here again on the left is differential outcomes in the placebo arm and in the drug treatment arm that if you were to just average these two you would not see the differences.
On the right is a really interesting study looking at alcohol among people with alcohol disorder, number of percent drinking days. And they looked at both COMT and OPRM1. And this is what Dr. Colloca was just talking about there seemed to be not just gene-placebo drug interactions but gene-gene drug placebo interactions. This is a complicated space. And I know we like things to be very simple. But I think what these data are showing is we need to pay more attention.
So let me give you another example because these -- you know, you could argue, okay, those are objective outcomes -- sorry, subjective outcomes. Let's take a look at the Women's Health Study. Arguably, one of the largest studies on aspirin versus placebo in history. 30,000 women were randomized to aspirin or placebo. And lo and behold, after 10 years of following them the p value was nonsignificant. There was no difference between drug and placebo.
So we went to this team, and we asked them, could we look at COMT because we had a hypothesis that COMT might modify the outcomes in the placebo arm and potentially differentially modify the treatments in the drug treatment arm. You might be saying that can't have anything to do with the placebo effect and we completely agree. This if we did find it would suggest that there might be something to do with the placebo response that is related to natural history. And I'm going to show you the data that -- what we found.
So when we compared the outcomes in the placebo arm to the aspirin arm, what we found was the met/met women randomized to placebo had the highest of everybody rates of cardiovascular disease. Which means the highest rates of myocardial infarction, stroke, revascularization and death from a cardiovascular disease cause. In contrast, the met/met women on aspirin had benefit, had a statistically significant reduction in these rates.
Conversely, the val/val women on placebo did the best, but the val/val women on aspirin had the highest rates, had significantly higher rates than the val/val women on placebo. What does this tell us? Well, we can't argue that this is a placebo effect because we don't have the control for placebo effects, which is a no treatment control.
But we can say that these are striking differences that, like I said before, if you don't pay attention to them, you miss the point that there are subpopulations for benefit or harm because of differential outcomes in the drug and placebo arms of the trial.
And so I'm going to keep going. There are other examples of this. We also partnered with a group at Brigham and Women's Hospital that had done the CAMP study, the Childhood Asthma Management Study. And in this study, they randomized patients to placebo, Budesonide or Nedocromil for five years and study asthma outcomes.
Now what I was showing you previously was candidate gene analyses. What this was, was a GWAS. We wanted to be agnostic and ask are there genes that modify the placebo outcomes and are these outcomes different in the -- when we look in the drug treatment arm. And so that little inset is a picture of all of the genes that were looked at in the GWAS. And we had a borderline genome Y significant hit called BBS9. And when we looked at BBS9 in the placebo arm, those white boxes at the top are the baseline levels of coughing and wheezing among these children. And in the gray are at the end of the treatment their level of coughing and wheezing.
And what you can see here is that participants with the AA genotype were the ones that benefited from the Bedenoside -- from placebo, whereas the GG, the patients with the GG genotype really there was no significant change.
Now, when we looked in the drug treatment arms, we were surprised to see that the outcomes were the same, of course, at baseline. There is no -- everybody is kind of the same. But you can see the differential responses depending on the genotype. And so, again, not paying attention to these gene drug/placebo interactions we miss another story that is happening here among our patients.
Now, I just want to -- I added this one because it is important just to realize that this is not just about gene-drug placebo. But these are also about epigenetic effects. And so here is the same study that I showed earlier on alcohol use disorder. They didn't just stop at looking at the polymorphisms or the genetic variants. This team also went so far as to look at methylation of OPRM1 and COMT.
So methylation is basically when the promoter region of a gene is basically blocked because it has a methyl group. It has methylation on some of the nucleotides in that region. So you can't make the protein as efficiently. And if you look on the right, what you can see in the three models that they looked at, they looked at other genes. They also looked at SLC6A3 that's involved in dopamine transport. And what you can see here is that there is significant gene by group by time interactions for all these three genes, these are candidate genes that they looked at.
And even more fascinating is their gene-by-gene interactions. Basically it is saying that you cannot say what the outcome is going to be unless you know the patient's or the participant's COMT or OPRM genotype A and also how methylated the promoter region of that -- of these genes are. So this makes for a very complicated story. And I know we like very simple stories.
But I want to say that I'm just adding to that picture that we had before to say that it's not just in terms of the gene's polymorphisms, but as Dr. Colloca just elegantly showed it is transcription as well as methylation that might be modifying what is happening in the drug treatment arm and the placebo treatment arm. And to add to this it might also be about the natural history of the condition.
So BBS9 is actually a gene that is involved in the cilia, the activity of the formation of the cilia which is really important in breathing in the nasal canal. And so, you can see that it is not just about what's happening in the moment when you are doing the placebo or drug or the clinical trial, it also might -- the genes might also be modifying where the patient starts out and how the patient might develop over time. So, in essence, we have a very complicated playground here.
But I think I have shown you that genetic variation, whether it is polymorphisms in the gene, gene-gene interactions or epigenetics or all of the above can modify the outcomes in placebo arms of clinical trials. And that this might be due to the genetic effects on placebo effects or the genetic effects on natural history. And this is something I think we need to understand and really pay attention to.
And I also think I've showed you, and these are just a few examples, there are many more. But genetic variation can differentially modify drugs and placebos and that these potential interactive effects really challenge this basic assumption of additivity that I would argue we have had for far too long and we really need to rethink.
TED KAPTCHUK: (Laughing) Very cool.
KATHRYN HALL: Hi, Ted.
TED KAPTCHUK: Oh, I didn't know I was on.
KATHRYN HALL: Yeah, that was great. That's great.
So in summary, can we use these gene-placebo drug interactions to improve clinical trials. Can we change our expectations about what is happening. And perhaps as we have been saying for the last two days, we don't need new drugs with clear physiological effects, what we need is to understand drug and placebo interactions and how they impact subpopulations and can reveal who benefits or is harmed by therapies.
And finally, as we started to talk about in the last talk, can we use drugs to boost placebo responses? Perhaps some drugs already do. Conversely, can we use drugs to block placebo responses? And perhaps some drugs already do.
So I just want to thank my collaborators. There was Ted Kaptchuk, one of my very close mentors and collaborators. And really, thank you for your time.
CRISTINA CUSIN: Thank you so much. It was a terrific presentation. And definitely Ted's captured laugh, it was just one of the best spontaneous laughs.
We have a couple of questions coming through the chat. One is about the heterogeneity of response in placebo arms. It is not uncommon to see quite a dispersion of responses at trials. Was that thought experiment, if one looks at the fraction of high responders in the placebo arms, would one expect to see, enrich for some of the genetic marker for and as placebo response?
KATHRYN HALL: I absolutely think so. We haven't done that. And I would argue that, you know, we have been having kind of quiet conversation here about Naloxone because I think as Lauren said yesterday that the findings of Naloxone is variable. Sometimes it looks like Naloxone is blocking placebo response and sometimes it isn't.
We need to know more about who is in that trial, right? Is this -- I could have gone on and showed you that there is differences by gender, right. And so this heterogeneity that is coming into clinical trials is not just coming from the genetics. It's coming from race, ethnicity, gender, population. Like are you in Russia or are you in China or are you in the U.S. when you're conducting your clinical trial? We really need to start unpacking this and paying attention to it. I think because we are not paying attention to it, we are wasting a lot of money.
CRISTINA CUSIN: And epigenetic is another way to consider traumatic experiences, adverse event learning. There is another component that we are not tracking accurately in clinical trials. I don't think this is a one of the elements routinely collected. Especially in antidepressant clinical trials it is just now coming to the surface.
KATHRYN HALL: Thank you.
CRISTINA CUSIN: Another question comes, it says the different approaches, one is GWAS versus candidate gene approach.
How do you start to think about genes that have a potential implication in neurophysiological pathways and choosing candidates to test versus a more agnostic U.S. approach?
KATHRYN HALL: I believe you have to do both because you don't know what you're going to find if you do a GWAS and it's important to know what is there.
At the same time, I think it's also good to test our assumptions and to replicate our findings, right? So once you do the GWAS and you have a finding -- for instance, our BBS9 finding would be amazing to replicate or to try and test in another cohort. But, of course, it is really difficult to do a whole clinical trial again. These are very expensive, and they last many years.
And so, you know, I think replication is something that is tough to do in this space, but it is really important. And I would do both.
CRISTINA CUSIN: Thank you. We got a little short on time. We are going to move on to the next speaker. Thank you so much.
FADEL ZEIDAN: Good morning. It's me, I imagine. Or good afternoon.
Let me share my screen. Yeah, so good morning. This is going to be a tough act to follow. Dr. Colloca and Dr. Hall's presentations were really elegant. So manage your expectations for mine. And, Ted, please feel free to unmute yourself because I think your laugh is incredibly contagious, and I think we were all were laughing as well.
So my name is Fadel Zeidan, I'm at UC San Diego. And I'll be discussing mostly unpublished data that we have that's under review examining if and how mindfulness meditation assuages pain and if the mechanism supporting mindfulness meditation-based analgesia are distinct from placebo.
And so, you know, this is kind of like a household slide that we all are here because we all appreciate how much of an epidemic chronic pain is and, you know, how significant it is, how much it impacts our society and the world. And it is considered a silent epidemic because of the catastrophic and staggering cost to our society. And that is largely due to the fact that the subjective experience of pain is modulated and constructed by a constellation of interactions between sensory, cognitive, emotional dimensions, genetics, I mean I can -- the list can go on.
And so what we've been really focused on for the last 20 years or so is to appreciate if there is a non-pharmacological approach, a self-regulated approach that can be used to directly assuage the experience of pain to acutely modify exacerbated pain.
And to that extent, we've been studying meditation, mindfulness-based meditation. And mindfulness is a very nebulous construct. If you go from one lab to another lab to another lab, you are going to get a different definition of what it is. But obviously my lab's definition is the correct one. And so the way that we define it is awareness of arising sensory events without reaction, without judgment.
And we could develop this construct, this disposition by practicing mindfulness-based meditation, which I'll talk about here in a minute. And we've seen a lot of -- and this is an old slide -- a lot of new evidence, converging evidence demonstrating that eight weeks of manualized mindfulness-based interventions can produce pretty robust improvements in chronic pain and opiate misuse. These are mindfulness-based stress reduction programs, mindfulness-oriented recovery enhancement, mindfulness-based cognitive therapy which are about eight weeks long, two hours of formalized didactics a week, 45 minutes a day of homework.
There is yoga, there is mental imagery, breathing meditation, walking meditation, a silent retreat and about a $600 tab. Which may not be -- I mean although they are incredibly effective, may not be targeting demographics and folks that may not have the time and resources to participate in such an intense program.
And to that extent and, you know, as an immigrant to this country I've noticed that we are kind of like this drive-thru society where, you know, we have a tendency to eat our lunches and our dinners in our cars. We're attracted to really brief interventions for exercise or anything really, pharmaceuticals, like ":08 Abs" and "Buns of Steel." And we even have things called like the military diet that promise that you'll lose ten pounds in three days without dying.
So we seemingly are attracted to these fast-acting interventions. And so to this extent we've worked for quite some time to develop a very user friendly, very brief mindfulness-based intervention. So this is an intervention that is about four sessions, 20 minutes each session. And participants are -- we remove all religious aspects, all spiritual aspects. And we really don't even call it meditation, we call it mindfulness-based mental training.
And our participants are taught to sit in a straight posture, close their eyes, and to focus on the changing sensations of the breath as they arise. And what we've seen is this repetitive practice enhances cognitive flexibility and the ability to -- flexibility and the ability to sustain attention. And when individual's minds drift away from focusing on the breath, they are taught to acknowledge distractive thoughts, feelings, emotions without judging themselves or the experience. Doing so by returning their attention back to the breath.
So there is really a one-two punch here where, A, you're focusing on the breath and enhancing cognitive flexibility; and, B, you're training yourself to not judge discursive events. And that we believe enhances emotion regulation. So quite malleable to physical training we would say mental training. Now that we have the advent of imaging, we can actually see that there are changes in the brain related to this.
But as many of you know, mindfulness is kind of like a household term now. It's all over our mainstream media. You know, we have, you know, Lebron meditating courtside. Oprah meditating with her Oprah blanket. Anderson Cooper is meditating on TV. And Time Magazine puts, you know, people on the cover meditating. And it's just all over the place.
And so these types of images and these types of, I guess, insinuations could elicit nonspecific effects related to meditation. And for quite some time I've been trying to really appreciate not is meditation more effective than placebo, although that's interesting, but does mindfulness meditation engage mechanisms that also are shared by placebo? So beliefs that you are meditating could elicit analgesic responses.
The majority of the manualized interventions in their manuals they use terms like the power of meditation, which I guarantee you is analgesic. To focus on the breath, we need to slow the breath down. Not implicit -- not explicitly, but it just happens naturally. And slow breathing can also reduce pain. Facilitator attention, social support, conditioning, all factors that are shared with other therapies and interventions but in particular are also part of meditation training.
So the question is because of all this, is mindfulness meditation merely -- or not merely after these two rich days of dialogue -- but is mindfulness meditation engaging processes that are also shared by placebo.
So if I apply a placebo cream to someone's calf and then throw them in the scanner versus asking someone to meditate, the chances are very high that the brain processes are going to be distinct. So we wanted to create a -- and validate an operationally matched mindfulness meditation intervention that we coined as sham mindfulness meditation. It's not sham meditation because it is meditation. It's a type of meditative practice called Pranayama.
But here in this intervention we randomize folks, we tell folks that they've been randomized to a genuine mindfulness meditation intervention. Straight posture, eyes closed. And every two to three minutes they are instructed to, quote-unquote, take a deep breath as we sit here in mindfulness meditation. We even match the time giving instructions between the genuine and the sham mindfulness meditation intervention.
So the only difference between the sham mindfulness and the genuine mindfulness is that the genuine mindfulness is taught to explicitly focus on the changing sensations of the breath without judgment. The sham mindfulness group is just taking repetitive deep, slow breaths. So if the magic part of mindfulness, if the active component of mindfulness is this nonjudgmental awareness, then we should be able to see disparate mechanisms between these.
And we also use a third arm, a book listening control group called the "Natural History of Selborne" where it's a very boring, arguably emotionally pain-evocating book for four days. And this is meant to control for facilitator time and -- sorry, facilitator attention and the time elapsed in the other group's interventions.
So we use a very high level of noxious heat to the back of the calf. And we do so because imaging is quite expensive, and we want to ensure that we can see pain-related processing within the brain. Here and across all of our studies, we use ten 12-second plateaus of 49 degrees to the calf, which is pretty painful.
And then we assess pain intensity and pain unpleasantness using a visual analog scale, where here the participants just see red the more they pull on the algometer the more in pain they are. But on the back, the numbers fluoresce where 0 is no pain and 10 is the worst pain imaginable.
So pain intensity can be considered like sensory dimension of pain, and pain unpleasantness could be more like I don't want to say pain affect but more like the bothersome component of pain, pain unpleasantness. So what we did was we combined all of our studies that have used the mindfulness, sham mindfulness in this book listing control, to see does mindfulness meditation engage is mindfulness meditation more effective than sham mindfulness meditation at reducing pain.
We also combined two different fMRI techniques: Blood oxygen dependent level signalling, bold, which allows us a higher temporal resolution and signal to noise ratio than, say, perfusion imaging technique and allows us to look at connectivity. However, meditation is also predicated on changes in respiration rate which could elicit pretty dramatic artifacts in the brain, breathing related artifacts explicitly related to CO2 output.
So using the perfusion based fMRI technique like arterial spin labeling is really advantageous as well, although it's not as temporally resolute as bold, it provides us a direct quantifiable measurement of cerebral blood flow.
So straight to the results. On the Y axis we have the pain ratings, and on the X axis are book listening controls sham mindfulness meditation, mindfulness meditation. Here are large sample sizes. Blue is intensity and red is unpleasantness. This is the post intervention fMRI scans where we see the first half of the scan to the second half of the scan our controlled participants are simply resting and pain just increases because of pain sensitization and being in a claustrophobic MRI environment.
And you can see here that sham mindfulness meditation does produce pretty significant reduction in pain intensity and unpleasantness, more than the control book. But mindfulness meditation is more effective than sham mindfulness and the controls at reducing pain intensity and pain unpleasantness.
There does seem to be some kind of additive component to the genuine intervention, although this is a really easy practice, the sham techniques.
So for folks that have maybe fatigue or cognitive deficits or just aren't into doing mindfulness technique, I highly recommend this technique, which is just a slow breathing approach, and it's dead easy to do.
Anyone that's practiced mindfulness for the first time or a few times can state that it can be quite difficult and what's the word? -- involving, right?
So what happened in the brain? These are our CBF maps from two studies that we replicated in 2011 and '15 where we found that higher activity, higher CBF in the right anterior insula, which is ipsilateral to the stimulation site and higher rostral anterior cingulate cortex subgenual ACC was associated with greater pain relief, pain intensity, and in the context of pain unpleasantness, higher over the frontal cortical activity was associated with lower pain, and this is very reproducible where we see greater thalamic deactivation predicts greater analgesia on the unpleasantness side.
These areas, obviously right entry insula in conjunction with other areas is associated with interoceptive processing awareness of somatic sensations. And then the ACC and the OFC are associated with higher order cognitive flexibility, emotional regulation processes. And the thalamus is really the gatekeeper from the brain -- I'm sorry, from the body to the brain. Nothing can enter the brain except unless it goes through the thalamus, except if it's the sense of smell.
So it's really like this gatekeeper of arising nociceptive information.
So the takehome here is that mindfulness is engaging multiple neural processes to assuage pain. It's not just one singular pathway.
Our gold studies were also pretty insightful. Here we ran a PPI analysis, psychophysiologic interaction analysis and this was whole brain to see what brain regions are associated with pain relief on the context of using the bold technique, and we find that greater ventral medial prefrontal cortical activity deactivation I'm sorry is associated with lower pain, and the vmPFC is a super evolved area that's associated with, like, higher order processes relating to self. It's one of the central nodes of the so called default mode network, a network supporting self referential processing. But in the context of the vmPFC, I like the way that Tor and Mathieu reflect the vmPFC as being more related to affective meaning and has a really nice paper showing that vmPFC is uniquely involved in, quote/unquote, self ownership or subjective value, which is particularly interesting for the context of pain because pain is a very personal experience that's directly related to the interpretation of arising sensations and what they mean to us.
And seemingly -- I apologize for the reverse inferencing here -- but seemingly mindfulness meditation based on our qualitative assessments as well is reducing the ownership or the intrinsic value, the contextual value of those painful sensations, i.e., they don't feel like they bother -- that pain is there but it doesn't bother our participants as much, which is quite interesting as a manipulation.
We also ran our connectivity analysis between the contralateral thalamus and the whole brain, and we found that greater decoupling between the contralateral thalamus and the precuneus, another central node of the default mode network predicted greater analgesia.
This is a really cool, I think, together mechanism showing that two separate analyses are indicating that the default mode network could be an analgesic system which we haven't seen before. We have seen the DMN involved in chronic pain and pain related exacerbations, but I don't think we've seen it as being a part of an analgesic, like being a pain relieving mechanism. Interestingly, the thalamus and precuneus together are the first two nodes to go offline when we lose consciousness, and they're the first two nodes to come back online when we recover from consciousness, suggesting that these two -- that the thalamus and precuneus are involved in self referential awareness, consciousness of self, things of this nature.
Again, multiple processes involved in meditation based pain relief which maybe gives rise to why we are seeing consistently that meditation could elicit long lasting improvements in pain unpleasantness, in particular, as compared to sensory pain. Although it does that as well.
And also the data gods were quite kind on this because these mechanisms are also quite consistent with the primary premises of Buddhist and contemplative scriptures saying that the primary principle is that your experiences are not you.
Not that there is no self, but that the processes that arise in our moment to moment experience are merely reflections and interpretations in judgments, and that may not be the true inherent nature of mind.
And so before I get into more philosophical discourse, I'm going to keep going for the sake of time. Okay.
So what happened with the sham mindfulness meditation intervention?
We did not find any neural processes predicted analgesia significantly and during sham mindfulness meditation. What did predict analgesia during sham mindfulness was slower breathing rate, which we've never seen before with mindfulness. We've never seen a significant or even close to significant relationship between mindfulness based meditation analgesia and slow breathing. But over and over we see that sham mindfulness based analgesia is related to slower breathing which provides us this really cool distinct process where kind of this perspective where mindfulness is engaging higher order top down type processes to assuage pain while sham mindfulness may be engaging this more bottom up type response to assuage pain.
I'm going to move on to some other new work, and this is in great collaboration with the lovely Tor Wager, and he's developed, with Marta and Woo, these wonderful signatures, these machine learned multivariate pattern signatures that are remarkably accurate at predicting pain over I think like 98, 99 percent.
His seminal paper, the Neurological Pain Signature, was published in the New England Journal of Medicine that showed that these signatures can predict nociceptive specific, in particular, for this particular, thermal heat pain with incredible accuracy.
And it's not modulated by placebo or affective components, per se. And then the SIIPS is a machine learned signature that is, as they put it, associated with cerebral contributions to pain. But if you look at it closely, these are markers that are highly responsive to the placebo response.
So the SIIPS can be used -- he has this beautiful pre print out, showing that it does respond with incredible accuracy to placebo, varieties of placebo.
So we used this MVPA to see if meditation engages signature supporting placebo responses.
And then Marta Ceko's latest paper with Tor published in Nature and Neuro found that the negative affect of signature predicts pain responses above and beyond nociceptive related processes. So this is pain related to negative affect, which again contributes to the multimodal processing of pain and how now we could use these elegant signatures to kind of disentangle which components of pain meditation and other techniques assuage. Here's the design.
We had 40 -- we combined two studies. One with bold and one with ASL. So this would be the first ASL study with signatures, with these MVPA signatures.
And we had the mindfulness interventions that I described before, the book listing interventions I described before and a placebo cream intervention which I'll describe now, all in response to 49 degrees thermal stimuli.
So across again all of our studies we use the same methods. And the placebo group -- I'll try to be quick about this -- this is kind of a combination of Luana Colloca, Don Price and Tor's placebo conditioning interventions where we administer 49 degrees -- we tell our participants that we're testing a new form of lidocaine, and the reason that it's new is that the more applications of this cream, the stronger the analgesia.
And so in the conditioning sessions, they come in, administer 49 degrees, apply and remove this cream, which is just petroleum jelly after 10 minutes, and then we covertly reduce the temperature to 48.
And then they come back in in session two and three, after 49 degrees and removing the cream, we lower the temperature to 47. And then on the last conditioning session, after we remove the cream, we lower the temperature to 46.5, which is a qualitatively completely different experience than 49.
And we do this to lead our participants to believe that the cream is actually working.
And then in a post intervention MRI session, after we remove the cream, we don't modulate the temperature, we just keep it at 49, and that's how we measured placebo in these studies. And then so here, again -- oops -- John Dean and Gabe are coleading this project.
Here, pain intensity on this axis, pain unpleasantness on that axis, controls from the beginning of the scan to the end of the scan significantly go up in pain.
Placebo cream was effective at reducing intensity and unpleasantness, but we see mindfulness meditation was more effective than all the conditions at reducing pain. The signatures, we see that the nociceptive specific signature, the controls go up in pain here.
No change in the placebo and mindfulness meditation you can see here produces a pretty dramatic reduction in the nociceptive specific signature.
The same is true for the negative affective pain signature. Mindfulness meditation uniquely modifies this signature as well which I believe this is one of the first studies to show something like this.
But it does not modulate the placebo signature. What does modulate the placebo signature is our placebo cream, which is a really nice manipulation check for these signatures.
So here, taken together, we show that mindfulness meditation, again, is engaging multiple processes and is reducing pain by directly assuaging nociceptive specific markers as well as markers supporting negative affect but not modulating placebo related signatures, providing further credence that it's not a placebo type response, and we're also demonstrating this granularity between a placebo mechanism that's not being shared by another active mechanism. While we all assume that active therapies and techniques are using a shared subset of mechanisms or processes with placebo, here we're providing accruing evidence that mindfulness is separate from a placebo.
I'll try to be very quick on this last part. This is all not technically related placebo, but I would love to hear everyone's thoughts on these new data we have.
So as we've seen elegantly that pain relief by placebo, distraction, acupuncture, transcranial magnetic stimulation, prayer, are largely driven by endogenous opioidergic release. And, yes, there are other systems. A prime other system is the (indiscernible) system, serotonergic system, dopamine. The list can go on. But it's considered by most of us that the endogenous opioidergic system is this central pain modulatory system.
And the way we do this is by antagonizing endogenous opioids by employing incredibly high administration dosage of naloxone.
And I think this wonderful paper by Ciril Etnes's (phonetic) group provides a nice primer on the appropriate dosages for naloxone to antagonize opiates. And I think a lot of the discussions here where we see differences in naloxone responses are really actually reflective of differences in dosages of naloxone.
It metabolizes so quickly that I would highly recommend a super large bolus with a maintenance infusion IV.
And we've seen this to be a quite effective way to block endogenous opioids. And across four studies now, we've seen that mindfulness based pain relief is not mediated by endogenous opioids. It's something else. We don't know what that something else is but we don't think it's endogenous opioids. But what if it's sex differences that could be driving these opioidergic versus non opioid opioidergic differences?
We've seen that females require -- exhibit higher rates of chronic pain than males. They are prescribed opiates at a higher rate than men. And when you control for weight, they require higher dosages than men. Why?
Well, there's excellent literature in rodent models and preclinical models that demonstrate that male rodents versus female -- male rodents engage endogenous opioids to reduce pain but female rodents do not.
And this is a wonderful study by Ann Murphy that basically shows that males, in response to morphine, have a greater latency and paw withdrawal when coupled with morphine and not so much with females.
But when you add naloxone to the picture, with morphine, the latency goes down. It basically blocks the analgesia in male rodents but enhances analgesia in female rodents.
We basically asked -- we basically -- Michaela, an undergraduate student doing an odyssey thesis asked this question: Are males and females in humans engaging in distinct systems to assuage pain?
She really took off with this and here's the design. We had heat, noxious heat in the baseline.
CRISTINA CUSIN: Doctor, you have one minute left. Can you wrap up?
FADEL ZEIDAN: Yep. Basically we asked, are there sex differences between males and females during meditation in response to noxious heat? And there are.
Baseline, just change in pain. Green is saline. Red is naloxone. You can see that with naloxone onboard, there's greater analgesia in females, and we reversed the analgesia. Largely, there's no differences between baseline in naloxone in males, and the males are reducing pain during saline.
We believe this is the first study to show something like this in humans. Super exciting. It also blocked the stress reduction response in males but not so much in females. Let me just acknowledge our funders. Some of our team. And I apologize for the fast presentation. Thank you.
CRISTINA CUSIN: Thank you so much. That was awesome.
We're a little bit on short on time.
I suggest we go into a short break, ten minute, until 1:40. Please continue to add your questions in Q&A. Our speakers are going to answer or we'll bring some of those questions directly to the discussion panel at the end of the session today. Thank you so much.
Measuring & Mitigating the Placebo Effect (continued)
CRISTINA CUSIN: Hello, welcome back. I'm really honored to introduce our next speaker, Dr. Marta Pecina. And she's going to talk about mapping expectancy-mood interactions in antidepressant placebo effects. Thank you so much.
MARTA PECINA: Thank you, Cristina. It is my great pleasure to be here. And just I'm going to switch gears a little bit to talk about antidepressant placebo effects. And in particular, I'm going to talk about the relationship between acute expectancy-mood neural dynamics and long-term antidepressant placebo effects.
So while we all know that depression is a very prevalent disorder, and just in 2020, Major Depressive Disorder affected 21 million adults in the U.S. and 280 million adults worldwide. And current projections indicate that by the year 2030 it will be the leading cause of disease burden globally.
Now, response rates to first-line treatments, antidepressant treatments are approximately 50%. And complete remission is only achieved in 30 to 35% of individuals. Also, depression tends to be a chronic disorder with 50% of those recovering from a first episode having an additional episode. And 80% of those with two or more episodes having another recurrence.
And so for patients who are nonresponsive to two intervention, remission rates with subsequent therapy drop significantly to 10 to 25%. And so, in summary, we're facing a disorder that is very resistant or becomes resistant very easily. And in this context, one would expect that antidepressant placebo effects would actually be low. But we all know that this is not the case. The response rate to placebos is approximately 40% compared to 50% response rates to antidepressants. And obviously this varies across studies.
But what we do know and learned yesterday as well is that response rates to placebos have increased approximately 7% over the last 40 years. And so these high prevalence of placebo response in depressions have significantly contributed to the current psychopharmacology crisis where large pharma companies have reduced at least in half the number of clinical trials devoted to CNS disorders.
Now, antidepressant placebo response rates among individuals with depression are higher than in any other psychiatric condition. And this was recently published again in this meta-analysis of approximately 10,000 psychiatric patients. Now, other disorders where placebo response rates are also prevalent are generalized anxiety disorder, panic disorders, HDHC or PTSD. And maybe less frequent, although still there, in schizophrenia or OCD.
Now, importantly, placebo effects appear not only in response to pills but also surgical interventions or devices, as it was also mentioned yesterday. And this is particularly important today where there is a very large development of device-based interventions for psychiatric conditions. So, for example, in this study that also was mentioned yesterday of deep brain stimulation, patients with resistant depression were assigned to six months of either active or some pseudo level DBS. And this was followed by open level DBS.
As you can see here in this table, patients from both groups improved significantly compared to baseline, but there were no significant differences between the two groups. And for this reason, DBS has not yet been approved by the FDA for depression, even though it's been approved for OCD or Parkinson's disease as we all know.
Now what is a placebo effect, that's one of the main questions of this workshop, and how does it work from a clinical neuroscience perspective? Well, as it's been mentioned already, most of what we know about the placebo effect comes from the field of placebo analgesia. And in summary, classical theories of the placebo effect have consistently argued that placebo effects results from either positive expectancies regarding the potential beneficial effects of a drug or classical conditioning where the pairing of a neutral stimulus, in this case the placebo pill, with an unconditioned stimulus, in this case the active drug, results in a conditioned response.
Now more recently, theories of the placebo effect have used computational models to predict placebo effects. And these theories posit that individuals update their expectancies as new sensory evidence is accumulated by signaling the response between what is expected and what is perceived. And this information is then used to refine future expectancies. Now these conceptual models have been incorporated into a trial-by-trial manipulation of both expectancies of pain relief and pain sensory experience. And this has rapidly advanced our understanding of the neural and molecular mechanisms of placebo analgesia.
And so, for example, in these meta analytic studies using these experiments they have revealed really two patterns of distinct activations with decreases in brain activity in regions involving brain processing such as the dorsal medial prefrontal cortex, the amygdala and the thalamus; and increases in brain activity in regions involving effective appraisal, such as the vmDFC, the nucleus accumbens, and the PAG.
Now what happens in depression? Well, in the field of antidepressant placebo effects, the long-term dynamics of mood and antidepressant responses have not allowed us to have such trial-by-trial manipulation of expectancies. And so instead researchers have used broad brain changes in the context of a randomized control trial or a placebo lead-in phase which has, to some extent, limited the progress of the field.
Now despite these methodological limitations of these studies, they provide important insights about the neural correlates of antidepressant placebo effects. In particular, from studies -- two early on studies we can see the placebo was associated with increased activations broadly in cortical regions and decreased activations in subcortical regions. And these deactivations in subcortical regions were actually larger in patients who were assigned to an SSRI drug treatment.
We also demonstrated that there is similar to pain, antidepressant placebo effects were associated with enhanced endogenous opiate release during placebo administration, predicting the response to open label treatment after ten weeks. And we have also -- we and others have demonstrated that increased connectivity between the salience network and the rostral anterior cingulate during antidepressant placebo effects can actually predict short-term and long-term placebo effects.
Now an important limitation, and as I already mentioned, is that this study is basically the delay mechanism of action of common antidepressant and this low dynamics of mood which really limit the possibility of actively manipulating antidepressant expectancies.
So to address this important gap, we develop a trial-by-trial manipulation of antidepressant expectancies to be used inside of the scanner. And the purpose was really to be able to further disassociate expectancy and mood dynamics during antidepressant placebo effects.
And so the basic structure of this test involved an expectancy condition where subjects are presented with a four-second infusion cue followed by an expectancy rating cue, and a reinforcement condition which consist of 20 seconds of some neurofeedback followed by a mood rating cue. Now the expectancy and the reinforcement condition map onto the classical theories of the placebo effect that I explained earlier.
During the expectancy condition, the antidepressant infusions are compared to periods of calibration where no drug is administered. And during the reinforcement condition, on the other hand, some neurofeedback of positive sign 80% of the time as compared to some neurofeedback of baseline sign 80% of the time. And so this two-by-two study design results in four different conditions. The antidepressant reinforced, the antidepressant not reinforced, the calibration reinforced, and the calibration not reinforced.
And so the cover story is that we tell participants that we are testing the effects of a new fast-acting antidepressant compared to a conventional antidepressant, but in reality, they are both saline. And then we tell them that they will receive multiple infusions of these drugs inside of the scanner while we record their brain activity which we call neurofeedback. So then patients learn that positive neurofeedback compared to baseline is more likely to cause mood improvement. But they are not told that the neurofeedback is simulated.
Then we place an intravenous line for the administration of the saline infusion, and we bring them inside of the scanner. For these kind of experiments we recruit individuals who are 18 through 55 with or without anxiety disorders and have a HAMD depression rating scale greater than 16, consistent with moderate depression. They're antidepressant medication free for at least 25 -- 21 days and then we use consenting procedures that involve authorized deception.
Now, as suspected, behavioral results during this test consistently show that antidepressant expectancies are higher during the antidepressant infusions compared to the calibration, especially when they are reinforced by positive sham neurofeedback. Now mood responses also are significantly higher during positive sham neurofeedback compared to baseline. But this is also enhanced during the administration of the antidepressant infusions.
Now interestingly, these effects are moderated by the present severity such that the effects of the test conditions and the expectancies and mood ratings are weaker in more severe depression even though their overall expectancies are higher, and their overall mood are lower.
Now at a neuron level, what we see is that the presentation of the infusion cue is associated with an increased activation in the occipital cortex and the dorsal attention network suggesting greater attention processing engaged during the presentation of the treatment cue. And similarly, the reinforcement condition revealed increased activations in the dorsal attention network with additional responses in the ventral striatum suggesting that individuals processed the sham positive neurofeedback cue as rewarding.
Now an important question for us was now that we can manipulate acute placebo -- antidepressant placebo responses, can we use this experiment to understand the mechanisms implicated in short-term and long-term antidepressant placebo effects. And so as I mentioned earlier, there was emerging evidence suggesting that placebo analgesic could be explained by computational models, in particular reinforcement learning.
And so we tested the hypothesis that antidepressant placebo effects could be explained by similar models. So as you know, under these theories, learning occurs when an experienced outcome differs from what is expected. And this is called the prediction error. And then the expected value of the next possible outcome is updated with a portion of this prediction error as reflected in this cue learning rule.
Now in the context of our experiment, model predicted expectancies for each of the four trial conditions would be updated every time the antidepressant or the calibration infusion cue is presented and an outcome, whether positive or baseline neurofeedback, is observed based on a similar learning rule.
Now this basic model was then compared against two alternative models. One which included differential learning rates to account for the possibility that learning would depend on whether participants were updating expectancies for the placebo or the calibration. And then an additional model to account for the possibility that subjects were incorporating positive mood responses as mood rewards.
And then finally, we constructed this additional model to allow the possibility of the combination of models two and three. And so using patient model comparison, we found that the model -- the fourth model, model four which included a placebo bias learning in our reinforcement by mood dominated all the other alternatives after correction for patient omnibus risk.
Now we then map the expected value and reward predictions error signals from our reinforcement learning models into our raw data. And what we found was that expected value signals map into the salience network raw responses; whereas reward prediction errors map onto the dorsal attention network raw responses. And so all together, the combination of our model-free and model-based results reveal that the processing of the antidepressant in patient cue increase activation in the dorsal attention network; whereas, the encoding of the expectancies took place in the salience network once salience had been attributed to the cue.
And then furthermore, we demonstrated that the reinforcement learning model predicted expectancies in coding the salience network triggered mood changes that are perceived as reward signals. And then these mood reward signals further reinforce antidepressant expectancies through the information of expectancy mood dynamics defined by models of reinforcement learning, an idea that could possibly contribute to the formation of long-lasting antidepressant placebo effects.
And so the second aim was really -- was going to look at these in particular how to use behavioral neuroresponses of placebo effects to predict long-term placebo effects in the context of a clinical trial. And so our hypothesis was that during placebo administration greater salient attribution to the contextual cue in the salience network would transfer to regions involved in mood regulation to induce mood changes. So in particular we hypothesized that the DMN would play a key role in belief-induced mood regulation.
And why the DMN? Well, we knew that activity in the rostral anterior cingulate, which is a key node of the DMN, is a robust predictor of mood responses to both active antidepressant and placebos, implying its involvement in nonspecific treatment response mechanisms. We also knew that the rostral anterior cingulate is a robust predicter of placebo analgesia consistent with its role in cognitive appraisals, predictions and evaluation. And we also had evidence that the SN to DMN functional connectivity appears to be a predictor of placebo and antidepressant responses over ten weeks of treatment.
And so in our clinical trial, which you can see the cartoon diagram here, we randomized six individuals to placebo or escitalopram 20 milligrams. And this table is just to say there were no significant differences between the two groups in regard to the gender, race, age, or depression severity. But what we found interesting is that there were also no significant differences in the correct belief assignment with 60% of subjects in each group approximately guessing that they were receiving escitalopram.
Now as you can see here, participants showed lower MADR scores at eight weeks in both groups. But there was no significant differences between the two groups. However, when split in the two groups by the last drug assignment belief, subjects with the drug assignment belief improved significantly compared to those with a placebo assignment belief.
And so the next question was can we use neuroimaging to predict these responses? And what we found was at a neural level during expectancy process the salience network had an increased pattern of functional connectivity with the DMN as well as with other regions of the brainstem including the thalamus. Now at the end -- we also found that increased SN to DMN functional connectivity predicted expectancy ratings during the antidepressant placebo fMRI task such that higher connectivity was associated with greater modulation of the task conditions on expectancy ratings.
Now we also found that enhanced functional connectivity between the SN and the DMN predicted the response to eight weeks of treatment, especially on individuals who believed that they were of the antidepressant group. Now this data supports that during placebo administration, greater salient attributions to the contextual cue is encoded in the salience network; whereas belief-induced mood regulation is associated with an increased functional connectivity between the SN and DMN and altogether this data suggest that enhancements to DMN connectivity enables the switch from greater salient attribution to the treatment cue to DMN-mediated mood regulation.
And so finally, and this is going to be brief, but the next question for us was can we modulate these networks to actually enhance placebo-related activity. And in particular, we decided to use theta burst stimulation which can potentiate or depotentiate brain activity in response to brief periods of stimulation. And so in this study participants undergo three counterbalance sessions of TBS with either continuous, intermittent, or sham known to depotentiate, potentiate, and have no effect.
So each TBS is followed by an fMRI session during the antidepressant placebo effect task which happens approximately an hour after stimulation. The inclusive criteria are very similar to all of our other studies. And our pattern of stimulation is pretty straightforward. We do two blocks of TBS. And during the first block stimulation intensity is gradually escalated in 5% increments in order to enhance tolerability. And during the second session the stimulation is maintained constant at 80% of the moderate threshold.
Then we use the modified cTBS session consisting of three stimuli applied at intervals of 30 hertz. We first repeat it at 6 hertz for a total of 600 stimuli in a continuous train of 33.3 seconds. Then we did the iTBS session consist of a burst of three stimuli applied at intervals of 50 hertz with bursts repeated at 5 hertz for a total of 600 stimulus during 192 seconds. We also use a sham condition where 50% of subjects are assigned to sham TBS simulating the iTBS stimulus pattern, and 50% are assigned to sham TBS simulating the cTBS pattern.
Now our target is the DMN which is the cortical target for the dorsal medial -- the cortical target for the DMN -- sorry, the dmPFC which is the cortical target for the DMN. And this corresponds to the -- and we found these effects based on the results from the antidepressant placebo fMRI task.
And so this target corresponds to our neurosynth scalp which is located 30% of the distance from the nasion-to-inion forward from the vertex and 5% left which corresponds to an EEG location of F1. And the connectivity map of these regions actually result in activation of the DMN. Now we can also show here the E-Field map of this target which basically demonstrates supports a nice coverage of the DMN.
And so what we found here is that the iTBS compared to sham and cTBS enhances the effect of the reinforcement condition of mood responses. And we also found that at a neural level iTBS compared to cTBS shows significant greater bold responses during expectancy processing within the DMN with sham responses in the middle but really not significantly different from iTBS. Now, increased bold responses in the ventral medial prefrontal cortex were associated with a greater effect of the task conditions of mood responses.
And so all together our results suggest that first trial-by-trial modulation of antidepressant expectancies effectively disassociates expectancy mood dynamics. Antidepressant expectancies are predicted by models of reinforcement learning and they're encoded in the salience network. We also showed that enhanced SN to DMN connectivity enables the switch from greater salient attribution to treatment cues to DMN-mediated mood regulation, contributing to the formation of acute expectancy-mood interactions and long-term antidepressant placebo effects. And iTBS potentiation of the DMN enhances placebo-induced mood responses and expectancy processing.
With this, I would just like to thank my collaborators that started this work with me at the University of Michigan and mostly the people in my lab and collaborators at the University of Pittsburgh as well as the funding agencies.
CRISTINA CUSIN: Wonderful presentation. Really terrific way of trying to untangle different mechanism in placebo response in depression, which is not an easy feat.
There are no specific questions in the Q&A. I would encourage everybody attending the workshop to please post your question to the Q&A. Every panelist can answer in writing. And then we will answer more questions during the discussion, but please don't hesitate.
I think I will move on to the next speaker. We have only a couple of minutes so we're just going to move on to Dr. Schmidt. Thank you so much. We can see your slides. We cannot hear you.
LIANE SCHMIDT: Can you hear me now?
CRISTINA CUSIN: Yes, thank you.
LIANE SCHMIDT: Thank you. So I'm Liane Schmidt. I'm an INSERM researcher and team leader at the Paris Brain Institute. And I'm working on placebo effects but understanding the appetitive side of placebo effects. And what I mean by that I will try to explain to you in the next couple of slides.
NIMH Staff: Can you turn on your video?
LIANE SCHMIDT: Sorry?
NIMH Staff: Can you please turn on your video, Dr. Schmidt?
LIANE SCHMIDT: Yeah, yes, yes, sorry about that.
So it's about the appetitive side of placebo effects because actually placebo effects on cognitive processes such as motivation and biases and belief updating because these processes actually play also a role when patients respond to treatment. And when we measure placebo effects, basically when placebo effects matter in the clinical setting.
And this is done at the Paris Brain Institute. And I'm working also in collaboration with the Pitie-Salpetriere Hospital Psychiatry department to get access to patients with depression, for example.
So my talk will be organized around three parts. On the first part, I will show you some data about appetitive placebo effects on taste pleasantness, hunger sensations and reward learning. And this will make the bridge to the second part where I will show you some evidence for asymmetrical learning biases that are more tied to reward learning and that could contribute actually or can emerge after fast-acting antidepressant treatment effects in depression.
And why is this important? I will try to link these two different parts, the first and second part, in the third part to elaborate some perspectives on the synergies between expectations, expectation updating through learning mechanisms, motivational mechanisms, motivational processes and drug experiences and which we can -- might harness actually by using computational models such as, for example, risk-reward Wagner models as Marta just showed you all the evidence for this in her work.
The appetitive side of placebo effects is actually known very well from the field of research in consumer psychology and marketing research where price labels, for example, or quality labels can affect decision-making processes and also experiences like taste pleasantness experience. And since we are in France, one of the most salient examples for these kind of effects comes from wine tasting. And many people have shown -- many studies have shown that basically the price of wine can influence how pleasant it tastes.
And we and other people have shown that this is mediated by activation in what is called the brain valuation systems or regions that encode expected and experienced reward. And one of the most prominent hubs in this brain valuation system is the ventral medial prefrontal cortex, what you see here on the SPM on the slide. That can explain, that basically translates these price label effects on taste pleasantness liking. And what is interesting is also that its sensitivity to monetary reward, for example, obtaining by surprise a monetary reward. It activates, basically the vmPFC activates when you obtain such a reward surprisingly.
And the more in participants who activate the vmPFC more in these kind of positive surprises, these are also the participants in which the vmPFC encoded more strongly the difference between expensive and cheap wines, which makes a nice parallel to what we know from placebo hyperalgesia where it has also been shown that the sensitivity of the reward system in the brain can moderate placebo analgesia with participants with higher reward sensitivity in the ventral striatum, for example, another region showing stronger placebo analgesia.
So this is to basically hope to let you appreciate that these effects parallel nicely what we know from placebo effects in the pain and also in disease. So we went further beyond actually, so beyond just taste liking which is basically experiencing rewards such as wine. But what could be -- could placebos also affect motivational processes per se? So when we, for example, want something more.
And one way to study is to study basic motivation such as, for example, hunger. It is long thought, for instance, eating behavior that is conceptualized to be driven by homeostatic markers, hormone markers such as Ghrelin and Leptin that signal satiety and energy stores. And as a function of these different hormonal markers in our blood, we're going to go and look for food and eat food. But we also know from the placebo effects on taste pleasantness that there is a possibility that our higher order beliefs about our internal states not our hormones can influence whether we want to eat food, whether we engage in these types of very basic motivations. And that we tested that, and other people also, that's a replication.
In the study where we gave healthy participants who came into the lab in a fasted state a glass of water. And we told them well, water sometimes can stimulate hunger by stimulating the receptors in your mouth. And sometimes you can also drink a glass of water to kill your hunger. And a third group, a control group was given a glass of water and told it's just water; it does nothing to hunger. And then we asked them to rate how hungry they feel over the course of the experiment. And it's a three-hour experiment. Everybody has fasted. And they have to do this food choice task in an fMRI scanner so they get -- everybody gets hungry over this three hours.
But what was interesting and what you see here on this rain cloud plot is that participants who believed or drank the water suggested to be a hunger killer increased in their hunger rating less than participants who believed the water will enhance their hunger. So this is a nice replication what we already know from the field; other people have shown this, too.
And the interesting thing is that it also affected this food wanting, this motivational process how much you want to eat food. So when people laid there in the fMRI scanner, they saw different food items, and they were asked whether they want to eat it or not for real at the end of the experiment. So it's incentive compatible. And what you see here is basically what we call stimulus value. So how much do you want to eat this food.
And the hunger sensation ratings that I just showed you before parallel what we find here. The people in the decreased hunger suggestion group wanted to eat the food less than in the increased hunger suggestion group, showing that it is not only an effect on subjective self-reports or how you feel your body signals about hunger. It's also about what you would actually prefer, what your subjective preference of food that is influenced by the placebo manipulation. And it's also influencing how your brain valuation system again encodes the value for your food preference. And that's what you see on this slide.
Slide two, you see the ventral medial prefrontal cortex. The yellow boxes that the more yellow they are, the stronger they correlate to your food wanting. And you see on the right side with the temporal time courses of the vmPFC that that food wanting encoding is stronger when people were on the increased hunger suggestion group than in the decreased hunger suggestion group.
So basically what I've showed you here is three placebo effects. Placebo effects on subjective hunger ratings, placebo effects on food choices, and placebo effects on how the brain encodes food preference and food choices. And you could wonder -- these are readouts. So these are behavioral readouts, neural readouts. But you could wonder what is the mechanism behind? Basically what is in between the placebo intervention here and basically the behavior feed and neural readout of this effect.
And one snippet of the answer to this question is when you look at the expectation ratings. For example, expectations have long been shown to be one of the mediators, the cognitive mediators of placebo effects across domains. And that's what we see here, too. Especially in the hunger killer suggestion group. The participants who believed that the hunger -- that the drug will kill their hunger more strongly were also those whose hunger increased less over the course of the experiment experience.
And this moderated activity in the region that you see here, which is called the medial prefrontal cortex, that basically activated when people saw food on the screen and thought about whether they want to eat it or not. And this region activated by that activity was positively moderated by the strength of the expectancy about the glass of water to decrease their hunger. So the more you expect that the water will decrease your hunger, the more the mPFC activates when you see food on the screen.
It's an interesting brain region because it's right between the ventral medial prefrontal cortex that encodes the value, the food preference, and the dorsal lateral prefrontal cortex. And it has been shown by past research to connect to the vmPFC when participants self-control, especially during food decision-making paradigms.
But another mechanism or another way to answer the question about the mechanism of how the placebo intervention can affect this behavior in neural effects is to use computational modelings to better understand the preference formation -- the preference formation basically. And one way is that -- is drift diffusion modeling. So these drift diffusion models come from perceptual research for understanding perception. And they are recently also used to better understand preference formation. And they assume that your preference for a yes or no food choice, for example, is a noisy accumulation of evidence.
And there are two types of evidence you accumulate in these two -- in these decision-making paradigms is basically how tasty and how healthy food is. How much you like the taste, how much you consider the health. And this could influence this loop of your evidence accumulation how rapidly basically you reach a threshold towards yes or no.
It could also be that the placebo and the placebo manipulation could influence this loop. But the model loops test several other hypotheses. It could be that the placebo intervention basically affected also just the threshold like that reflects how carefully you made the decision towards a yes or no choice. It could be your initial bias; that is, basically initially you were biased towards a yes or a no response. Or it could be the nondecision time which reflects more sensory motor integration.
And the answer to this question is basically that three parameters were influenced by the placebo manipulation. Basically how much you integrated healthiness and tastiness in your initial starting bias. So you paid more attention to the healthiness when you believed that you were on a hunger killer. And more the tastiness when you believed that you were on a hunger enhancer. And similarly, you were initially biased towards accepting food more when participants believed they were on a hunger enhancer than on a hunger killer.
Interestingly, so this basically shows that this decision-making process is biased by the placebo intervention and basically also how much you filter information that is most relevant. When you are hungry, basically taste is very relevant for your choices. When you are believing you are less hungry, then you have more actually space or you pay less attention to taste, but you can also pay attention more to healthiness of food.
And so the example that shows that this might be a filtering of expectation-relevant information is to use psychophysiologic interaction analyzers that look basically at the brain activity in the vmPFC, that's our seed region. Where in the brain does it connect when people, when participants see food on a computer screen and have to think about whether they want to eat this food or not?
And what we observed there that's connected to the dlPFC, the dorsal lateral prefrontal cortex region. And it's a region of interest that we localized first to be sure it is actually a region that is inter -- activating through an interference resolution basically when we filter -- have to filter information that is most relevant to a task in a separate Stroop localizer task.
So the vmPFC connects stronger to this dlPFC interference resolution region and this is moderated especially in the decreased hunger suggestion group by how much participants considered the healthiness against the tastiness of food.
To wrap this part up, it's basically that we replicated findings from previous studies about appetitive placebo effects by showing that expectancies about efficiency of a drink can affect hunger sensations. How participants make -- form their food preferences, make food choices. And value encoding in the ventral medial prefrontal cortex.
But we also provided evidence for underlying neurocognitive mechanisms that involve the medial prefrontal cortex that is moderated by the strengths of the hunger expectation. That the food choice formation is biased in the form of attention-filtering mechanism toward expectancy congruent information that is taste for an increased hunger suggestion group, and healthiness for a decreased hunger suggestion group. And this is implemented by regions that are linked to interference resolution but also to valuation preference encoding.
And so why should we care? In the real world, it is not very relevant to provide people with deceptive information about hunger-influencing ingredients of drinks. But studies like this one provide insights into cognitive mechanisms of beliefs about internal states and how these beliefs can affect the interoceptive sensations and also associated motivations such as economic choices, for example.
And this can actually also give us insights into the synergy between drug experiences and outcome expectations. And that could be harnessed via motivational processes. So translated basically via motivational processes. And then through it maybe lead us to better understand active treatment susceptibility.
And I'm going to elaborate on this in the next part of the talk by -- I'm going a little bit far, coming a little bit far, I'm not talking about or showing evidence about placebo effects. But yes -- before that, yes, so basically it is.
Links to these motivational processes have long been suggested actually to be also part of placebo effects or mechanisms of placebo effect. And that is called the placebo-reward hypothesis. And that's based on findings in Parkinson's disease that has shown that when you give Parkinson's patients a placebo but tell them it's a dopaminergic drug, then you can measure dopamine in the brain. And the dopamine -- especially the marker for dopamine, its binding potential decreases. That is what you see here on this PET screen -- PET scan results.
And that suggests that the brain must have released endogenous dopamine. And dopamine is very important for expectations and learning. Basically learning from reward. And clinical benefit is the kind of reward that patients expect. So it might -- it is possible that basically when a patient expects reward clinical benefit, its brain -- their brain releases dopamine in remodulating that region such as the vmPFC or the ventral striatum.
And we have shown this in the past that the behavioral consequence of such a nucleus dopamine release under placebo could be linked to reward learning, indeed. And what we know is that, for example, that Parkinson patients have a deficit in learning from reward when they are off dopaminergic medication. But this normalizes when they are under active dopaminergic medication.
So we wondered if based on these PET studies under placebo, the brain releases dopamine, does this also have behavior consequences on their reward learning ability. And that is what you see here on the screen on the right side on the screen is that the Parkinson patients basically tested on placebo shows similar reward learning abilities as under active drug.
And this again was also underpinned by increased correlation of the ventral medial prefrontal cortex. Again, this hub of the brain valuation system to the learned reward value. That was stronger in the placebo and active drug condition compared to baseline of drug condition.
And I want to make now this -- a link to another type of disease where also the motivation is deficitary, and which is depression. And depression is known to be maintained or is sympathized to be maintained by this triad of very negative beliefs about the world, the future and one's self. Which is very insensitive to belief disconfirming information, especially if the belief disconfirming information is positive, so favorable. And this has been shown by cognitive neuroscience studies to be reflected by a thought of like of good news/bad news bias or optimism biases and belief updating in depression. And this good news/bad news bias is basically a bias healthy people have to consider favorable information that contradicts initial negative beliefs more than negative information.
And this is healthy because it avoids reversing of beliefs. And it also includes a form of motivational process because good news have motivational salience. So it should be more motivating to update beliefs about the future, especially if these beliefs are negative, then when we learn that our beliefs are way too negative and get information about that disconfirms this initial belief. But depressed patients, they like this good news/bad news bias. So we wonder what happens when patients respond to antidepressant treatments that give immediate sensory evidence about being on an antidepressant.
And these new fast-acting antidepressants such as Ketamine, these types of antidepressants that patients know right away whether they got the treatment through dissociative experiences. And so could it be that this effect or is it a cognitive model of depression. So this was the main question of the study. And then we wondered again what is the computational mechanism. And is it linked again also, as shown in the previous studies, to reward learning mechanisms, so biased updating of beliefs. And is it linked to clinical antidepressant effects and also potentially outcome expectations makes the link to placebo effects.
So patients were given the -- were performing a belief updating task three times before receiving Ketamine infusions. And then after first infusion and then one week after the third infusion, each time, testing time we measured the depression with the Montgomery-Asberg Depression Rating Scale. And patients performed this belief updating task where they were presented with different negative life events like, for example, getting a disease, losing a wallet here, for example.
And they were asked to estimate their probability of experiencing this life event in the near future. And they were presented with evidence about the contingencies of this event in the general population, what we call the base rate. And then they had the possibility to update their belief knowing now the base rate.
And this is, for example, a good news trial where participants initially overestimated the chance for losing a wallet and then learn it's much less frequent than they initially thought. Updates, for example, 15%. And in a bad news trial, it's you initially underestimated your probability of experiencing this adverse life event. And if you have a good news/bad news bias, well, you're going to consider this information to a lesser degree than in a good news trial.
And that's what -- exactly what happens in the healthy controls that you see on the left most part of the screen. I don't know whether you can see the models, but basically we have the belief updating Y axis. And this is healthy age-matched controls to patients. And you can see updating of the good news. Updating of the bad news. We tested the participants more than two times within a week. You can see the bias. There is a bias that decreases a little bit with more sequential testing in the healthy controls. But importantly, in the patients the bias is there although before Ketamine treatment.
But it becomes much more stronger after Ketamine treatment. It emerged basically. So patients become more optimistically biased after Ketamine treatment. And this correlates to the MADRS scores. Patients who improve more with treatment are also those who show a stronger good news/bad news bias after one week of treatment.
And we wondered again about the computational mechanisms. So one way to get at this using a Rescoria-Wagner model reward reinforcement learning model that basically assumes that updating is proportional to your surprise which is called the estimation error.
The difference between the initial estimate and the base rate. And this is weighted by learning rate. And the important thing here is the learning rate has got two components, a scaling parameter and an asymmetry parameter. And the asymmetry parameter basically weighs in how much the learning rate varies after good news, after positive estimation error, than after negative estimation errors.
And what we can see that in healthy controls, there is a stronger learning rate for positive estimation errors and less stronger for negative estimation errors translating this good news/bad news bias. It's basically an asymmetrical learning mechanism. And in the patients, the asymmetrical learning is non-asymmetrical before Ketamine treatment. And it becomes asymmetrical as reflected in the learning rates after Ketamine treatment.
So what we take from that is basically that Ketamine induced an optimism bias. But an interesting question is whether -- basically what comes first. Is it basically the improvement in the depression that we measured with the Montgomery-Asberg Depression Rating Scale, or is it the optimism bias that emerged and that triggered basically. Since it's a correlation, we don't know what comes first.
And an interesting side effect or aside we put in the supplement was that in 16 patients, it's a very low sample size, the expectancy about getting better also correlated to the clinical improvement after Ketamine treatment. We have two expectancy ratings here about the efficiency about Ketamine and also what patients expect their intensity of depression will be after Ketamine treatment.
And so that suggested the clinical benefit is kind of in part or synergistically seems to interact with the drug experience that emerges that generates an optimism bias. And to test this more, we continued data collection just on the expectancy ratings. And basically wondered how the clinical improvement after first infusion links to the clinical improvement after third infusion.
And we know from here that patients improve after first infusion are also those that improved after a third infusion. But is it mediated by their expectancy about the Ketamine treatment? And that's what we indeed found is that basically the more patients expected to get better, the more they got better after one week of treatment. But it mediated this link between the first drug experience and the later drug experiences and suggested there might not be an additive effect as other panelist members today already put forward today, it might be synergetic link.
And one way to get at these synergies is basically again use computational models. And this idea has been around although yesterday that basically there could be self-fulfilling prophesies that could contribute to the treatment responsiveness and treatment adherence. And these self-fulfilling prophesies are biased symmetrically learning mechanisms that are more biased when you have positive treatment experiences, initial positive treatment experiences, and then might contribute how you adhere to the treatment in the long term and also how much you benefit from it in the long term. So it's both drug experience and an expectancy.
And so this is nonpublished work where we played with this idea basically using a reinforcement learning model. This is also very inspired by we know from placebo analgesia. Tor and Luana Kuven, they have a paper on showing that self-fulfilling prophecies can be harnessed with biased patient and reinforcement learning models. And the idea of these models is that there are two learning rates, alpha plus and alpha minus. And these learning rates rate differently into the updating of your expectation after drug experience.
LIANE SCHMIDT: Okay, yeah, I'm almost done.
So rate differently on these drug experiences and expectations as a function of whether the initial experience was congruent to your expectations. So a positive experience, then a negative one. And here are some simulations of this model. I'm showing this basically that your expectation is getting more updated the more bias, positively biased you are. Then when you are negatively biased. And these are some predictions of the model concerning depression improvement.
To wrap this up, the conclusion about this is that there seems to be asymmetrical learning that can capture self-fulfilling prophesies and could be a mechanism that translates expectations and drug experiences potentially across domains from placebo hypoalgesia to antidepressant treatment responsiveness. And the open question is obviously to challenge these predictions of these models more with empirical data in pain but also in mood disorders as Marta does and as we do also currently at Cypitria where we test the mechanisms of belief updating biases in depression with fMRI and these mathematical models.
And this has a direct link implication because it could help us to better understand how these fast-acting antidepressants work and what makes patients adhere to them and get responses to them. Thank you for your attention. We are the control-interoception-attention team. And thank you to all the funders.
CRISTINA CUSIN: Fantastic presentation. Thank you so much. Without further ado, let's move on to the next speaker. Dr. Greg Corder.
GREG CORDER: Did that work? Is it showing?
GREG CORDER: Awesome, all right. One second. Let me just move this other screen. Perfect. All right.
Hi, everyone. My name is Greg Corder. I'm an Assistant Professor at the University of Pennsylvania. I guess I get to be the final scientific speaker in this session over what has been an amazing two-day event. So thank you to the organizers for also having me get the honor of representing the entire field of preclinical placebo research as well.
And so I'm going to give a bit of an overview, some of my friends and colleagues over the last few years and then tell you a bit about how we're leveraging a lot of current neuroscience technologies to really identify the cell types and circuits building from, you know, the human fMRI literature that's really honed in on these key circuits for expectations, belief systems as well as endogenous antinociceptive symptoms, in particular opioid cell types.
So the work I'm going to show from my lab has really been driven by these two amazing scientists. Dr. Blake Kimmey, an amazing post-doc in the lab. As well as Lindsay Ejoh, who recently last week just received her D-SPAN F99/K00 on placebo circuitry. And we think this might be one of the first NIH-funded animal projects on placebo. So congratulations, Lindsay, if you are listening.
Okay. So why use animals, right? We've heard an amazing set of stories really nailing down the specific circuits in humans leveraging MRI, fMRI, EEG and PET imaging that give us this really nice roadmap and idea of how beliefs in analgesia might be encoded within different brain circuits and how those might change over times with different types of patient modeling or updating of different experiences.
And we love this literature. We -- in the lab we read it in depth as best as we can. And we use this as a roadmap in our animal studies because we can take advantage of animal models that really allow us to dive deep into the very specific circuits using techniques like that on the screen here from RNA sequencing, electrophysiology really showing that those functional measurements in fMRI are truly existent with the axons projecting from one region to another.
And then we can manipulate those connections and projections using things like optogenetics and chemogenetics that allow us really tight temporal coupling to turn cells on and off. And we can see the effects of that intervention in real time on animal behavior. And that's really the tricky part is we don't get to ask the animals do you feel pain? Do you feel less pain? It's hard to give verbal suggestions to animals.
And so we have to rely on a lot of different tricks and really get into the heads of what it's like to be a small prey animal existing in a world with a lot of large monster human beings around them. So we really have to be very careful about how we design our experiments. And it's hard. Placebo in animals is not an easy subject to get into. And this is reflected in the fact that as far as we can tell, there is only 24 published studies to date on placebo analgesia in animal models.
However, I think this is an excellent opportunity now to really take advantage of what has been the golden age of neuroscience technologies exploding in the last 10-15 years to revisit a lot of these open questions about when are opioids released, are they released? Can animals have expectations? Can they have something like a belief structure and violations of those expectations that lead to different types of predictions errors that can be encoded in different neural circuits. So we have a chance to really do that.
But I think the most critical first thing is how do we begin to behaviorally model placebo in these preclinical models. So I want to touch on a couple of things from some of my colleagues. So on the left here, this is a graph that has been shown on several different presentations over the past two days from Benedetti using these tourniquet pain models where you can provide pharmacological conditioning with an analgesic drug like morphine to increase this pain tolerance.
And then if it is covertly switched out for saline, you can see that there is an elevation in that pain tolerance reflective of something like a placebo analgesic response overall. And this is sensitive to Naloxone, the new opioid receptor antagonist, suggesting endogenous opioids are indeed involved in this type of a placebo-like response.
And my colleague, Dr. Matt Banghart, at UCSD has basically done a fantastic job of recapitulating this exact model in mice where you can basically use morphine and other analgesics to condition them. And so if I just kind of dive in a little bit into Matt's model here.
You can have a mouse that will sit on a noxious hot plate. You know, it's an environment that's unpleasant. You can have contextual cues like different types of patterns on the wall. And you can test the pain behavior responses like how much does the animal flick and flinch and lick and bite and protect itself to the noxious hot plate.
And then you can switch the contextual cues, provide an analgesic drug like morphine, see reductions in those pain behaviors. And then do the same thing in the Benedetti studies, you switch out the morphine for saline, but you keep the contextual cues. So the animal has effectively created a belief that when I am in this environment, when I'm in this doctor's office, I'm going to receive something that is going to reduce my perceptions of pain.
And, indeed, Matt sees a quite robust effect here where this sort of placebo response is -- shows this elevated paw withdrawal latency indicating that there is endogenous nociception occurring with this protocol. And it happens, again, pretty robustly. I mean most of the animals going through this conditioning protocol demonstrate this type of antinociceptive behavioral response. This is a perfect example of how we can leverage what we learn from human studies into rodent studies for acute pain.
And this is also really great to probe the effects of placebo in chronic neuropathic pain models. And so here this is Dr. Damien Boorman who was with Professor Kevin Key in Australia, now with Lauren Martin in Toronto.
And here Damien really amped up the contextual cues here. So this is an animal who has had an injury to the sciatic nerve with this chronic constriction injury. So now this animal is experiencing something like a tonic chronic neuropathic pain state. And then once you let the pain develop, you can have the animals enter into this sort of placebo pharmacological conditioning paradigm where animals will go onto these thermal plates, either hot or cool, in these rooms that have a large amount of visual tactile as well as odorant cues. And they are paired with either morphine or a controlled saline.
Again, the morphine is switched for saline on that last day. And what Damien has observed is that in a subset of the animals, about 30%, you can have these responder populations that show decreased pain behavior which we interpret as something like analgesia overall. So overall you can use these types of pharmacological conditionings for both acute and chronic pain.
So now what we're going to do in our lab is a bit different. And I'm really curious to hear the field's thoughts because all -- everything I'm about to show is completely unpublished. Here we're going to use an experimenter-free, drug-free paradigm of instrumental conditioning to instill something like a placebo effect.
And so this is what Blake and Lindsay have been working on since about 2020. And this is our setup in one of our behavior rooms here. Our apparatus is this tiny little device down here. And everything else are all the computers and optogenetics and calcium imaging techniques that we use to record the activity of what's going on inside the mouse's brain.
But simply, this is just two hot plates that we can control the temperature of. And we allow a mouse to freely explore this apparatus. And we can with a series of cameras and tracking devices plot the place preference of an animal within the apparatus. And we can also record with high speed videography these highly conserved sort of protective recuperative pain-like behaviors that we think are indicative of the negative affect of pain.
So let me walk you through our little model here real quick. Okay. So we call this the placebo analgesia conditioning assay or PAC assay. So here is our two-plate apparatus here. So plate number one, plate number two. And the animal can always explore whichever plate it wants. It's never restricted to one side. And so we have a habituation day, let the animal familiarize itself. Like oh, this is a nice office, I don't know what's about to happen.
And then we have a pretest. And in this pretest, importantly, we make both of these plates, both environments a noxious 45-degree centigrade. So this will allow the animal to form an initial expectation that the entire environment is noxious and it's going to hurt. So both sides are noxious. Then for our conditioning, this is where we actually make one side of the chamber non-noxious. So it's just room temperature. But we keep one side noxious. So now there is a new expectation for the animal that it learns that it can instrumentally move its body from one side to the other side to avoid and escape feeling pain.
And so we'll do this over three days, twice per day. And then on our post tester placebo day we make both environments hot again. So now we'll start the animal off over here and the animals will get to freely choose do they want to go to the side that they expect should be non-noxious? Or what happens? So what happens?
Actually, if you just look at the place preference for this, over the course of conditioning we can see that the animals will, unsurprisingly, choose the environment that is non-noxious. And they spend 100% of their time there basically. But when we flip the plates or flip the conditions such that everything is noxious on the post test day, the animals will still spend a significant amount of time on the expected analgesia side. So I'm going to show you some videos here now and you are all going to become mouse pain behavior experts by the end of this.
So what I'm going to show you are both side by side examples of conditioned and unconditioned animals. And try to follow along with me as you can see what the effect looks like. So on this post test day. Oh, gosh, let's see if this is going to -- here we go. All right. So on the top we have the control animal running back and forth. The bottom is our conditioned animal.
And you'll notice we start the animal over here and it's going to go to the side that it expects it to not hurt. Notice the posture of the animals. This animal is sitting very calm. It's putting its entire body down on the hot plate. This animal, posture up, tail up. It's running around a little bit frantically. You'll notice it start to lick and bite and shake its paws. This animal down here might have a couple of flinches so it's letting you know that some nociception is getting into the nervous system overall.
But over the course of this three-minute test, the animals will rightly choose to spend more time over here. And if we start to quantify these types of behaviors that the animals are doing in both conditions, what we find is that there is actually a pretty significant reduction in these nociceptive behaviors. But it's not across the entire duration of this placebo day or post test day.
So this trial is three minutes long. And what we see is that this antinociceptive and preference choice only exists for about the first 90 seconds of this assay. So this is when the video I just showed, the animal goes to the placebo side, it spends a lot of its time there, does not seem to be displaying pain-like behaviors.
And then around 90 seconds, the animal -- it's like -- it's almost like the belief or the expectation breaks. And at some point, the animal realizes oh, no, this is actually quite hot. It starts to then run around and starts to show some of the more typical nociceptive-like behaviors. And we really like this design because this is really, really amenable to doing different types of calcium imaging, electrophysiology, optogenetics because now we have a really tight timeline that we can observe the changing of neural dynamics at speeds that we can correlate with some type of behavior.
Okay. So what are those circuits that we're interested in overall that could be related to this form of placebo? Again, we like to use the human findings as a wonderful roadmap. And Tor has demonstrated, and many other people have demonstrated this interconnected distributed network involving prefrontal cortex, nucleus accumbens, insula, thalamus, as well as the periaqueductal gray.
And so today I'm going to talk about just the periaqueductal gray. Because there is evidence that there is also release of endogenous opioids within this system here. And so we tend to think that the placebo process and the encoding, whatever that is, the placebo itself is likely not encoded in the PAG. The PAG is kind of the end of the road. It's the thing that gets turned on during placebo and we think is driving the antinociceptive or analgesic effects of the placebo itself.
So the PAG, for anyone who's not as familiar, we like it because it's conserved across species. We look at in a mouse. There's one in a human. So potentially it's really good for translational studies as well. It has a very storied past where it's been demonstrated that the PAG subarchitecture has these beautiful anterior to posterior columns that if you electrically stimulate different parts of PAG, you can produce active versus passive coping mechanisms as well as analgesia that's dependent on opioids as well as endocannabinoids.
And then the PAG is highly connected. Both from ascending nociception from the spinal cord as well as descending control systems from prefrontal cortex as well as the amygdala. So with regard to opioid analgesia. If you micro infuse morphine into the posterior part of the PAG, you can produce an analgesic effect in rodents that is across the entire body. So it's super robust analgesia from this very specific part of the PAG.
If you look at the PAG back there and you do some of these techniques to look for histological indications that the mu opioid receptor is there, it is indeed there. There is a large amount of mu opioid receptors, it's OPRM1. And it's largely on glutamatergic neurons. So the excitatory cells, not the inhibitory cells. They are on some of them.
And as far as E-phys data goes as well, we can see that the mu opioid receptor is there. So DAMGOs and opioid agonist. We can see activation of inhibitory GIRK currents in those cells. So the system is wired up for placebo analgesia to happen in that location. Okay. So how are we actually going to start to tease this out? By finding these cells where they go throughout the brain and then understanding their dynamics during placebo analgesia.
So last year we teamed up with Karl Deisseroth's lab at Stanford to develop a new toolkit that leverages the genetics of the opioid system, in particular the promoter for the mu opioid receptor. And we were able to take the genetic sequence for this promoter and package it into adeno associated viruses along with a range of different tools that allow us to turn on or turn off cells or record their activity. And so we can use this mu opioid receptor promoter to gain genetic access throughout the brain or the nervous system for where the mu opioid receptors are. And we can do so with high fidelity.
This is just an example of our mu opioid virus in the central amygdala which is a highly mu opioid specific area. But so Blake used this tool using the promoter to drive a range of different trans genes within the periaqueductal gray. And right here, this is the G camp. So this is a calcium indicator that allows us to in real time assess the calcium activity of PAG mu opioid cells.
And so what Blake did was he took a mouse, and he recorded the nociceptive responses within that cell type and found that the mu opioid cell types are actually nociceptive. They respond to pain, and they do so with increasing activity to stronger and stronger and more salient and intense noxious stimuli. So these cells are actually nociceptive.
And if we look at a ramping hot plate, we can see that those same mu opioid cell types in the PAG increase the activity as this temperature on this hot plate increases. Those cells can decrease that activity if we infuse morphine.
Unsurprisingly, they express the mu opioid receptor and they're indeed sensitive to morphine. If we give naltrexone to block the mu opioid receptors, we can see greater activity to the noxious stimuli, suggesting that there could be an opioid tone or some type of an endogenous opioid system that's keeping this system in check, that it's repressing its activity. So when we block it, we actually enhance that activity. So it's going to be really important here. The activity of these mu opioid PAG cells correlates with affective measures of pain.
When animals are licking, shaking, biting, when it wants to escape away from noxious stimuli, that's when we see activity within those cells. So this is just correlating different types of behavior when we see peak amplitudes within those cell types. So let me skip that real quick.
Okay. So we have this ability to look and peek into the activity of mu opioid cell types. Let's go back to that placebo assay, our PAC assay I mentioned before. If we record from the PAG on that post test day in an animal that has not undergone conditioning, when the plates are super hot, we see a lot of nocioceptive activity in these cells here. They're bouncing up and down.
But if we look at the activity of the nociception in an animal undergoing placebo, what we see is there's a suppression of neural activity within that first 90 seconds. And this actually does seem to extinguish within the lighter 90 seconds. So kind of tracks along with the behavior of those animals. When they're showing anti nocioceptive behavior, that's when those cells are quiet.
When the pain behavior comes back, that's when those cell types are ramping up. But what about the opioids too? Mu opioid receptor cell type's decreasing activity. What about the opioids themselves here? The way to do this in animals has been to use microdialysis, fantastic technique but it's got some limitations to it. This is a way of sampling peptides in real time and then using liquid chromatography to tell if the protein was present. However, the sampling rate is about 10 minutes.
And in terms of the brain processing, 10 minutes might as well be an eternity. If we're talking about milliseconds here. But we want to know what these cells here and these red dots are doing. These are the enkephaliner cells in the PAG. We needed revolution in technologies. One of those came several years ago from Dr. Lin Tian, who developed some of the first sensors for dopamine. Some of you may have heard of it. It's called D-Light.
This is a version of D-Light. But it's actually an enkephalin opioid sensor. What Lin did to genetically engineer this is to take the delta opioid receptor, highly select it for enkephalin, and then link it with this GFP molecule here such that when enkephalin binds to the sensor it will fluoresce.
We can capture that florescence with microscopes that we implant over the PAG and we can see when enkephalin is being released with subsecond resolution. And so what we did for that is we want to see if enkephalin is indeed being released onto those mu opioid receptor expressing pain encoding neurons in the PAG. What I showed you before is that those PAG neurons, they ramp up their activity as the nociception increases, a mouse standing on a hot plate. We see nociception ramp up. What do you all think happened with the opoids?
It wasn't what we expected. It actually drops. So what we can tell is that there's a basal opioid tone within the PAG, but that as nociception increases, acute nociception, we see a decrease suppression of opioid peptide release.
We think this has to do with stuff that Tor has published on previously that the PAG is more likely involved in updating prediction errors. And this acute pain phenomenon we think is reflective of the need to experience pain to update your priors about feeling pain and to bias the selection of the appropriate behaviors, like affect related things to avoid pain. However, what happens in our placebo assay?
We actually see the opposite. So if we condition animals to expect pain relief within that PAC assay, we actually see an increase from the deltoid sensor suggesting that there is an increase in enkephalin release post conditioning. So there can be differential control of the opioid system within this brain region. So this next part is the fun thing you can do with animals. What if we just bypassed the need to do the placebo assay?
If we know that we just need to cause release of enkephalin within the PAG to produce pain relief, we could just directly do that with optigenetics. So we tried to us this animal that allows us to put a red light sensitive opsin protein into the enkephalinergic interneurons into the PAG.
When we shine red light on top of these cells, they turn on and they start to release their neurotransmitters. These are GABAergic and enkephalinergic. So they're dumping out GABA and now dumping out enkephalin into the ERG. We can visualize that using the Delta Light sensor from Lin Tien.
So here is an example of optogenetically released enkephalin within the PAG over 10 minutes. The weird thing that we still don't fully understand is that this signal continues after the optogenetic stimulation. So can we harness the placebo effect in mice? At least it seems we can. So if we turn on these cells strongly, cause them to release enkephalin and put animals back on these ramping hot plate tests we don't see any changes in the latency to detect pain, but we see specific ablation or reductions in these affective motivational pain like behaviors overall. Moderator: You have one minute remaining.
GREGORY CORDER: Cool. In this last minutes, people are skeptical. Can we actually test these higher order cognitive processes in animals? And for anyone who is not a behavioral preclinical neural scientist, you might not be aware there's an absolute revolution happening in behavior with the use of deep learning modules that can precisely and accurately quantify animal behavior. So this is an example of a deep learning tracking system.
We've built the Light Automated Pain Evaluator that can capture a range of different pain related behaviors fully automated without human intervention whatsoever that can be paired with brain reporting techniques like calcium imaging, that allow us to fit a lot of different computational models to understand what the activity of single neurons might be doing, let's say, in the cingulate cortex that might be driving that placebo response.
We can really start to tie now in at single cell resolution the activity of prefrontal cortex to drive these placebo effects and see if that alters anti nocioceptive behavior endogenously. I'll stop there and thank all the amazing people, Blake, Greg, and Lindsay, who did this work, as well as all of our funders and the numerous collaborators who have helped us do this. So thank you.
CRISTINA CUSIN: Terrific talk. Thank you so much. We're blown away. I'll leave the discussion to our two moderators. They're going to gather some of the questions from the chat and some of their own questions for all the presenters from today and from yesterday as well.
TED KAPTCHUK: Matt, you start gathering questions. I got permission to say a few moments of comments. I wanted to say this is fantastic. I actually learned an amazing amount of things. The amount of light that was brought forward about what we know about placebos and how we can possibly control placebo effects, how we can possibly harness placebo effects.
There was so much light and new information. What I want to do in my four minutes of comments is look to the future. What I mean by that is -- I want to give my comments and you can take them or leave them but I've got a few minutes.
What I want to say is we got the light, but we didn't put them together. There's no way we could have. We needed to be more in the same room. How does this fit in with your model? It's hard to do. What I mean by putting things together is I'll give you an example. In terms of how do we control placebo effects in clinical trials. I not infrequently get asked by the pharmaceutical industry, when you look at our placebo data -- we just blew it. Placebo was good as or always as good as the drug.
And the first thing I say is I want to talk to experts in that disease. I want to know the natural history. I want to know how you made your entry criteria so I can understand regression to the mean.
I want to know what's the relationship of the objective markers and subjective markers so I can begin to think about how much is the placebo response. I always tell them I don't know. If I knew how to reduce -- increase the difference between drug and placebo I'd be a rich man, I wouldn't be an academic. What I usually wind up saying is, get a new drug. And they pay me pretty well for that. And the reason is that they don't know anything about natural history. We're trying to harness something, and I just want to say -- I've done a lot of natural history controls, and that's more interesting than the rest of the experiments because they're unbelievable, the amount of improvement people show entering the trial without any treatment.
I just want to say we need to look at other things besides the placebo effect. We want to control the placebo response in a randomized control trial. I want to say that going forward. But I also want to say that we need a little bit of darkness. We need to be able to say, you know, I disagree with you. I think this other data, and one of the things I've learned doing placebo reach there's a paper that contradicts your paper real quickly and there's lots of contradictory information. It's very easy to say you're wrong, and we don't say it enough.
I want to take one example -- please forgive me -- I know that my research could be said that, Ted, you're wrong. But I just want to say something. Consistently in the two days of talk everyone talks about the increase of the placebo response over time. No one refers to the article published in 2022 in BMJ, first author was Mark Stone and senior author was Irving Kirsch. And they analyzed all FDA Mark Stone is in the Division of Psychiatry at CDER at the FDA. They analyzed all data of placebo controlled trials in major depressive disorder. They had over 230 trials, way more than 70,000 patients, and they analyzed the trend over time, in 1979 to the present, the publication. There was no increase in the placebo effect.
Are they right or are other people right? Nothing is one hundred percent clear right now and we need to be able to contradict each other when we get together personally and say, I don't think that's right, maybe that's right. I think that would help us. And the last thing I want to say is that some things were missing from the conference that we need to include in the future. We need to have ethics. Placebo is about ethics. If you're a placebo researcher in placebo controlled trials, that's an important question:
What are we talking about in terms of compromising ethics? There's no discussion that we didn't have time but in the future, let's do that.
And the last thing I would say is, we need to ask patients what their experience is. I've got to say I've been around for a long time. But the first time I started asking patients what their experiences were, they were in double blind placebo or open label placebo, I did it way after they finished the trial, the trial was over, and I actually took notes and went back and talked to people. They told me things I didn't even know about. And we need to have that in conferences. What I want to say, along those lines, is I feel so much healthier because I'm an older person, and I feel with this younger crowd here is significantly younger than me.
Maybe Matt and I are the same age, I don't know, but I think this is really one of the best conferences I ever went to. It was real clear data. We need to do lots of other things in the future. So with that, Matt, feed me some questions.
MATTHEW RUDORFER: Okay. Thanks. I didn't realize you were also 35. But okay. [LAUGHTER].
MATTHEW RUDORFER: I'll start off with a question of mine. The recent emergence of intravenous ketamine for resistant depression has introduced an interesting methodologic approach that we have not seen in a long time and that is the active placebo. So where the early trials just used saline, more recently we have seen benzodiazapine midazolam, while not mimicking really the full dissociative effect that many people get from ketamine, but the idea is for people to feel something, some kind of buzz so that they might believe that they're on some active compound and not just saline. And I wonder if the panel has any thoughts about the merits of using an active placebo and is that something that the field should be looking into more?
TED KAPTCHUK: I'm going to say something. Irving Kirsch published a meta analysis of H studies that used atropine as a control in depression studies. He felt that it made it difficult to detect a placebo drug difference. But in other meta analysis said that was not true. That was common in the '80s. People started thinking about that. But I have no idea how to answer your question.
MICHAEL DETKE: I think that's a great question. And I think in the presentations yesterday about devices, Dr. Lisanby was talking about the ideal sham. And I think it's very similar, the ideal active placebo would have none of the axia of the drug, of the drug in question, but would have, you know, exactly the same side effects and all other features, and of course that's attractive, but of course we probably would never have a drug that's exactly like that. I think midazolam was a great thing to try with ketamine. It's still not exactly the same. But I'd also add that it's not black and white. It's not like we need to do this with ketamine and ignore it for all of our other drugs. All of our drugs have side effects.
Arguably, if you do really big chunks, like classes of relatively modern antidepressants, antipsychotics and the psychostimulants, those are in order of bigger effect sizes in clinical trials, psychostimulants versus anti psychotics, versus -- and they're also in the order of roughly, I would argue, of unblinding, of functional unblinding. And in terms of more magnitude, Zyprexa will make you hungry. And also speed of onset of some of the adverse effects, stimulants and some of the Type II -- the second generation and beyond -- anti psychotics, they have pretty noticeable side effects for many subjects and relatively rapidly. So I think those are all important features to consider.
CRISTINA CUSIN: Dr. Schmidt?
LIANE SCHMIDT: I think using midazolam could give, like, some sensory sensations so the patients actually can say there's some effect on the body like immediately. But this raises actually a question whether these dissociations we observe in some patients of ketamine infusions we know have, will play a role for the antidepressant response. It's still an open question. So I don't have the answer to that question. And I think with midazolam doesn't really induce dissociations. I don't know, maybe you can isolate the dissociations you get on ketamine. But maybe even patients might be educated, expecting scientific reaction experiences and basically when they don't have -- so they make the midazolam experience something negative. So yeah, just self fulfilling prophesies might come into play.
CRISTINA CUSIN: I want to add for five seconds. Because I ran a large ketamine clinic. We know very little about cyto placebo maintaining an antidepressant response while the dissociation often wears off over time. It's completely separate from the anti depressant effect. We don't have long term placebo studies. The studies are extremely short lived and we study the acute effect. But we don't know how to sustain or how to maintain, what's the role of placebo effect in long term treatments. So that's another field that really is open to investigations. Dr. Rief.
WINFRIED RIEF: Following up on the issue of active placebos. I just want to mention that we did a study comparing active placebos to passive placebos and showing that active placebos are really more powerful. And I think the really disappointing part of this news is that it questions the blinding of our typical RCTs comparing antidepressants versus placebos because many patients who are in the active group or the tracked group, they perceive these onset effects and this will further boost the placebo mechanisms in the track group that are not existing in the passive placebo group. This is a challenge that further questions the validity of our typical RCTs.
CRISTINA CUSIN: Marta.
MARTA PECINA : Just a quick follow up to what Cristina was saying, too, that we need to clarify whether we want to find an active control for the dissociative effects or for the antidepressive effects. I think the approach will be very different. And this applies to ketamine but also psychodelics because we're having this discussion as well. So when thinking about how to control for or how to blind or how we just -- these treatments are very complicated. They have multiple effects. We just need to have the discussion of what are we trying to blind because the mechanism of action of the blinding drug will be very different.
TED KAPTCHUK: Can I say something about blinding? Robertson, who is the author of the 1970 -- no -- 1993 New England Journal paper saying that there's no that the placebo effect is a myth.
In 2022, published in BMJ, the largest -- he called it a mega meta analysis on blinding. And he took 144 randomized control trials that included nonblinded evidence on the drug versus blinded evidence of the drug. I'm not going to tell you the conclusion because it's unbelievable. But you should read it because it really influences -- it would influence what we think about blinding. That study was just recently replicated on a different set of patients with procedures in JAMA Surgery three months ago. And blinding like placebo is more complicated than we think. That's what I wanted to say.
MATTHEW RUDORFER: Another clinical factor that's come up during our discussion has been the relationship of the patient to the provider that we saw data showing that a warm relationship seemed to enhance therapeutic response, I believe, to most interventions. And I wonder what the panel thinks about the rise on the one hand of shortened clinical visits now that, for example, antidepressants are mostly given by busy primary care physicians and not specialists and the so called med check is a really, kind of, quickie visit, and especially since the pandemic, the rise of telehealth where a person might not ever even meet their provider in person, and is it possible we're on our way to where a clinical trial could involve, say, mailing medication every week to a patient, having them do their weekly ratings online and eliminating a provider altogether and just looking at the pharmacologic effect?
I mean, that probably isn't how we want to actually treat people clinically, but in terms of research, say, early phase efficacy, is there merit to that kind of approach?
LUANA COLLOCA: I'll comment on this, Dr. Rudorfer. We're very interested to see how the telemedicine or virtual reality can affect placebo effects, and we're modeling in the lab placebo effects induced via, you know, in person interaction.
There's an Avatar and virtual reality. And actually we found placebo effects with both the settings. Or whether, when we look at empathy, the Avatar doesn't elicit any empathy in the relationship. We truly need the in person connection to have empathy. So that suggests that our outcome that are affected by having in person versus telemedicine/para remote interactions, but yet the placebo effects persist in both the settings. The empathy is differently modulated and the empathy mediated, interestingly in our data, placebo effects only in the in person interactions. There is still a value in telemedicine. Effects that bypass empathy completely in competence.
MATTHEW RUDORFER: Dr. Hall.
KATHRYN HALL: Several of the large studies, like the Women's Health Study, Physicians' Health Study and, more recently, Vital, they did exactly that, where they mail these pill packs. And I mean, the population, obviously, is clinicians. So they are very well trained and well behaved. And they follow them for years but there's very little contact with the providers, and you still have these giant -- I don't know if you can call them placebo effects -- but certainly many of these trials have not proven to be more effective, the drugs they're studying, than placebo.
MATTHEW RUDORFER: Dr. Atlas.
LAUREN ATLAS: I wanted to chime in briefly on this important question. I think that the data that was presented yesterday in terms of first impressions of providers is relevant for this because it suggests that even when we use things like soft dot (phonetic) to select physicians and we have head shots (phonetic), that really we're making these decisions about who to see based on these kinds of just first impressions and facial features and having the actual interactions by providers is critical for sort of getting beyond that kind of factor that may drive selection. So I think if we have situations where there's reduced chances to interact, first of all, people are bringing expectations to the table based on what they know about the provider and then you don't really have the chance to build on that without the actual kind of therapeutic alliance. That's why I think, even though our study was done in an artificial setting, it really does show how we make these choices when there are bios for physicians and things available for patients to select from. I think there's a really important expectation being brought to the table before the treatment even occurs.
MATTHEW RUDORFER: Thanks. Dr. Lisanby.
SARAH “HOLLY” LISANBY: Thanks for raising this great question, Matt. I have a little bit of a different take on it. Equity in access to mental health care is a challenge. And the more that we can leverage technology to provide and extend the reach of mental health care the better. And so telemedicine and telepsychiatry, we've been thrust into this era by the pandemic but it existed before the pandemic as well. And it's not just about telepsychotherapy or teleprescription from monitoring pharmacotherapy, but digital remote neuromodulation is also a thing now. There are neuromodulation interventions that can be done at home that are being studied, and so there have been trials on transcranial direct current stimulation at home with remote monitoring. There are challenges in those studies differentiating between active and sham. But I think you're right in that we may have to rethink how do we control remote studies when the intensity of the clinician contact is very different, but I do think that we should explore these technologies so that we can extend the reach and extend access to research and to care for people who are not able to come into the research lab setting.
TED KAPTCHUK: May I add something on this? It's also criticizing myself. In 2008, I did this very nice study showing you could increase the doctor/patient relationship. And as you increase it, the placebo effect got bigger and bigger, like a dose response. A team in Korea that I worked with replicated that. I just published that replication.
The replication came out with the exact opposite results. The less doctor/patient relationship, the less intrusive, the less empathy got better effects. We're dealing with very complicated culturally constructed issues, and I just want to put it out there, the sand is soft. I'm really glad that somebody contradicted a major study that I did.
LUANA COLLOCA: Exactly. The central conference is so critical, what we observed in one context in one country, but even within the same in group or out group can be completely different in Japan, China or somewhere else. So the Americas, South Africa. So we need larger studies and more across country collaborations.
MATTHEW RUDORFER: Dr. Schmidt.
LIANE SCHMIDT: I just wanted to raise a point not really like -- it's more like a comment, like there's also very interesting research going on in the interactions between humans and robots, and usually humans treat robots very badly. And so I wonder what could be like -- here we focus on very human traits, like empathy, competence, what we look at. But when it comes to artificial intelligence, for example, and when we have to interact with algorithms, basically, like all these social interactions might completely turn out completely different, actually, and all have different effects on placebo effects. Just a thought.
MATTHEW RUDORFER: Dr. Rief.
WINFRIED RIEF: Yesterday, I expressed a belief for showing more warmth and competence, but I'll modify it a little bit today because I think the real truth became quite visible today, and that is that there is an interaction between these non specific effect placebo effects and the track effect. In many cases, at least. We don't know whether there are exceptions from this rule, but in many cases we have an interaction. And to learn about the interaction, we instead need study designs that modulate track intake versus placebo intake, but they also modulate the placebo mechanisms, the expectation mechanisms, the context of the treatment. And only if we have these 2 by 2 designs, modulating track intake and modulating context and psychological factors, then we learn about the interaction. You cannot learn about the interaction if you modulate only one factor.
And, therefore, I think what Luana and others have said that interact can be quite powerful and effective in one context but maybe even misleading in another context. I think this is proven. We have to learn more about that. And all the studies that have been shown from basic science to application that there could be an interaction, they're all indicating this line and to this necessity that we use more complex designs to learn about the interaction.
MATTHEW RUDORFER: Yes. And the rodent studies we've seen, I think, have a powerful message for us just in terms of being able to control a lot of variables that are just totally beyond our control in our usual human studies. It always seemed to me, for example, if you're doing just an antidepressant versus placebo trial in patients, well, for some people going into the clinic once a week to get ratings, that might be the only day of the week that they get up and take a shower, get dressed, have somebody ask them how they're doing, have some human interaction. And so showing up for your Hamilton rating could be a therapeutic intervention that, of course, we usually don't account for in the pharmacotherapy trial. And the number of variables really can escalate in a hurry when we look at our trials closely.
TED KAPTCHUK: Tor wants to say something.
TOR WAGER: Thanks, Ted.
I wanted to add on to the interaction issue, which came up yesterday, which Winfried and others just commented on, because it seems like it's really a crux issue. If the psychosocial or expectation effects and other things like that are entangled with specific effects so that one can influence the other and they might interact, then, yeah, we need more studies that independently manipulate specific drug or device effects and other kinds of psychological effects independently. And I wanted to bring this back up again because this is an idea that's been out here for a long time. I think the first review on this was in the '70s, like '76 or something, and it hasn't really been picked up for a couple of reasons. One, it's hard to do the studies. But second, when I talk to people who are in industry and pharma, they are very concerned about changing the study designs at all for FDA approval.
And since we had some, you know, FDA and regulatory perspectives here yesterday, I wanted to bring that up and see what people think, because I think that's been a big obstacle. And if it is, then that may be something that would be great for NIH to fund instead of pharma companies because then there's a whole space of drugs, psychological or neurostimulation psychological interactions, that can be explored.
MATTHEW RUDORFER: We also had a question. Yesterday there was discussion in a naloxone trial in sex differences in placebo response. And wonder if there's any further thoughts on studies of sex differences or diversity in general in placebo trials. Yes.
LUANA COLLOCA: We definitely see sex differences in placebo effect, and I show also, for example, women responded to arginine vasopressin in a way that we don't observe in men.
But also you asked about diversity. Currently actually in our paper just accepted today where we look at where people are living, the Maryland states, and even the location where they are based make a difference in placebo effects. So people who live in the most distressed, either the greatest Baltimore area, tended to have lower placebo effects as compared to a not distressful location. And we define that the radius of the criteria and immediately it's a race but we take into account the education, the income and so on. So it is interesting because across studies consistently we see an impact of diversity. And in that sense, I echo, listen to the comment that we need to find a way to reach out to these people and truly improve access and the opportunity for diversity. Thank you for asking.
MATTHEW RUDORFER: Thank you. Another issue that came up yesterday had to do with the pharmacogenomics. And there was a question or a question/comment about using candidate approaches and are they problematic.
KATHRYN HALL: What approaches.
MATTHEW RUDORFER: Candidate genes.
KATHRYN HALL: I think we have to start where we are. I think that the psychiatric field has had a really tough time with genetics. They've invested a lot and, sadly, don't have as much to show for it as they would like to. And I think that that has really tainted this quest for genetic markers of placebo and related studies, these interaction factors. But it's really important to not, I think, to use that to stop us from looking forward and identifying what's there. Because when you start to scratch the surface, there are interactions. You can see them. They're replete in the literature. And what's really fascinating is everybody who finds them, they don't see them when they report their study. And even some of these vasopressin studies, not obviously, Tor, yours, but I was reading one the other day where they had seen tremendous differences by genetics in response to arginine vasopressin. And they totally ignored what they were seeing in placebo and talked about who responds to drug. And so I think that not only do we need to start looking for what's happening, we need to start being more open minded and paying attention to what we're seeing in the placebo arm and accounting for that, taking that into account to understand what we're seeing across a trial in total.
CRISTINA CUSIN: I'll take a second to comment on sufficient selection and trying to figure out, depending on the site who are the patients who went there, treatment and depression clinical trial. If we eliminate from the discussion professional patient and we think about the patients who are more desperate, patients who don't have access to care, patients who are more likely to have psychosocial stressors or the other extreme, there are patients who are highly educated. The trials above and they search out, but they're certainly not representative of the general populations we see in the clinical setting.
They are somewhat different. And then if you think about the psychedelics trial, they go from 5,000 patients applying for a study and the study ends up recruiting 20, 30. So absolutely not representative of the general population we see in terms of diversity, in terms of comorbidities, in terms of psychosocial situations. So that's another factor that adds to the complexity of differentiating what happens in the clinical setting versus artificial setting like a research study. Tor.
MATTHEW RUDORFER: The question of who enters trials and I think the larger issue of diagnosis in general has, I think, really been a challenge to the field for many years. Ted and I go back a ways, and just looking at depression, of course, has dominated a lot of our discussion these last couple of days, with good reason. Now I realize the good database, my understanding is that the good database of placebo controlled trials go back to the late '90s, is what we heard yesterday. And if you go back further, the tricyclic era not only dealt with different medications, which we don't want to go back to, but if you think about practice patterns then, on the one hand, the tricyclics, most nonspecialists steered clear of, they required a lot of hands on. They required titration slowly up. They had some concerning toxicities, and so it was typical that psychiatrists would prescribe them but family docs would not. And that also had the effect of a naturalistic screening, that is, people would have to reach a certain level of severity before they were referred to a psychiatrist to get a prescription for medication.
More mildly ill people either wound up, probably inappropriately, on tranquilizers or no treatment at all and moderately to severely ill people wound up on tricyclics, and of course inpatient stays were common in those days, which again was another kind of screening. So it was the sort of thing, I mean, in the old days I heard of people talk about, well, you could, if you go to the inpatient board, you could easily collect people to be in clinical trial and you kind of knew that they were vetted already. That they had severe depression, the general sense was that the placebo response would be low. Though there's no real evidence for that. But the thing is, once we had the SSRIs on the one hand, the market vastly expanded because they're considered more broad spectrum. People with milder illness and anxiety disorders now are appropriate candidates and they're easier to dispense. The concern about overdose is much less, and so they're mostly prescribed by nonspecialists. So it's the sort of thing where we've seen a lot of large clinical trials where it doesn't take much to reach the threshold for entry, being if I go way back and this is just one of my personal concerns over many years the finer criteria, which I think were the first good set of diagnostic criteria based on data, based on literature, those were published in 1972 to have a diagnosis of major depression, called for four weeks of symptoms. Actually, literally, I think it said one month.
DSM III came out in 1980 and it called for two weeks of symptoms. I don't know -- I've not been able to find any documentation of how the one month went to two weeks, except that the DSM, of course, is the manual that's used in clinical practice. And you can understand, well, you might not want to have too high a bar to treat people who are seeking help. But I think one of the challenges of DSM, it was not meant as a research manual. Though that's often how it's used. So ever since that time, those two weeks have gotten reified, and so my point is it doesn't take much to reach diagnostic criteria for DSM, now, 5TR, major depression. So if someone is doing a clinical trial of an antidepressant, it is tempting to enroll people who meet, honestly meet those criteria but the criteria are not very strict. So I wonder whether that contributes to the larger placebo effect that we see today.
End of soapbox. The question -- I'd like to revisit an excellent point that Dr. Lisanby raised yesterday which has to do with the research domain criteria, the RDOC criteria. I don't know if anyone on the panel has had experience in using that in any trials and whether you see any merit there. Could RDOC criteria essentially enrich the usual DSM type clinical criteria in terms of trying to more finely differentiate subtypes of depression, might respond differently to different treatments.
MODERATOR: I think Tor has been patient on the hand off. Maybe next question, Tor, I'm not sure if you had comments on previous discussion.
TOR WAGER: Sure, thanks. I wanted to make a comment on the candidate gene issue. And I think it links to what you were just saying as well, doctor, in a sense. I think it relates to the issue of predicting individual differences in placebo effects and using that to enhance clinical trials, which has been really sort of a difficult issue. And in genetics, I think what's happened, as many of us know, is that there were many findings on particular candidate genes, especially comped and other particular set of genes in Science and Nature, and none of those really replicated when larger GWA studies started being done. And the field of genetics really focused in on reproducibility and replicability in one of our sample sizes. So I think my genetics colleagues tell me something like 5,000 is a minimum for even making it into their database of genetic associations. And so that makes it really difficult to study placebo effects in sample sizes like that. And at the same time, there's been this trend in psychology and in science, really, in general, towards reproducibility and replicability that probably in part are sort of evoked by John Ioannidis's provocative claims that most findings are false, but there's something really there.
There's been many teams of people who have tried to pull together, like Brian Nosek's work with Open Science Foundation, and many lab studies to replicate effects in psychology with much higher power. So there's this sort of increasing effort to pull together consortia to really test these things vigorously. And I wonder if -- we might not have a GWA study of placebo effects in 100,000 people or something, which is what would convince a geneticist that there's some kind of association. I'm wondering what the ways forward are, and I think one way is to increasingly come together to pull studies or do larger studies that are pre registered and even registered reports which are reviewed before they're published so that we can test some of these associations that have emerged in these what we call early studies of placebo effects.
And I think if we preregister and found something in sufficiently large and diverse samples, that might make a dent in convincing the wider world that essentially there is something that we can use going forward in clinical trials. And pharma might be interested in, for example, as well. That's my take on that. And wondering what people think.
KATHRYN HALL: My two cents. I completely agree with you. I think the way forward is to pull our resources to look at this and not simply stop -- I think when things don't replicate, I think we need to understand why they don't replicate. I think there's a taboo on looking beyond, if you prespecified it and you don't see it, then it should be over. I think in at least this early stage, when we're trying to understand what's happening, I think we need to allow ourselves deeper dives not for action but for understanding.
So I agree with you. Let's pull our resources and start looking at this. The other thing I would like to point out that's interesting is when we've looked at some of these clinical trials at the placebo arm, we actually learn a lot about natural history. We just did one in Alzheimer's disease and in the placebo arm the genome wide significant hit was CETP, which is now a clinical target in Alzheimer's disease. You can learn a lot by looking at the placebo arms of these studies not just about whether or not the drug is working or how the drug is working, but what's happening in the natural history of these patients that might change the effect of the drug.
TED KAPTCHUK: Marta, did you have something to say; you had your hand up.
MARTA PECINA: Just a follow up to what everybody is saying. I do think the issue of individualability is important. I think that one thing that maybe kind of explains some of the things that was also saying at the beginning that there's a little bit of lack of consistency or a way to put all of these findings together. The fact that we think about it as a one single placebo effect and we do know that there's not one single placebo effect, but even within differing clinical conditions is the newer value placebo effect the same in depression as it is in pain?
Or are there aspects that are the same, for example, expectancy processing, but there's some other things that are very specific to the clinical condition, whether it's pain processing, mood or some others. So I think we face the reality of use from a neurobiology perspective that a lot of the research has been done in pain and still there's very little being done at least in psychiatry across many other clinical conditions that we just don't know. And we don't really even know if the placebo how does the placebo effect look when you have both pain and depression, for example?
And so those are still very open questions that kind of reflect our state, right, that we're making progress but there's a lot to do.
TED KAPTCHUK: Winfried, did you want to say something? You have your hand up.
WINFRIED RIEF: I wanted to come back to the question of whether we really understand this increase of placebo effects. I don't know whether you have (indiscernible) for that. But I'm more like a scientist I can't believe that people are nowadays more reacting to placebos than they did 20 years ago. So there might be other explanations for this effect, like we changed the trial designs. We have more control visits maybe nowadays compared to 30 years ago, but there could be also other factors like publication bias which was maybe more frequent, more often 30 years ago than it is nowadays with the need for greater registration. So there are a lot of methodological issues that could explain this increase of placebo effects or of responses in the placebo groups. I would be interested whether you think that this increase is well explained or what your explanations are for this increase.
TED KAPTCHUK: Winfried, I want to give my opinion. I did think about this issue. I remember the first time it was reported in scientists in Cleveland, 40, 50 patients, and I said, oh, my God, okay, and the newspapers had it all over: The placebo effect is increasing. There's this boogie man around, and everyone started believing it. I've been consistently finding as many papers saying there's no -- I've been collecting them. There's no change over time there are changes over time. When I read the original article, I said, of course there's differences. The patients that got recruited in 1980 were different than the patients in 1990 or 2010. They were either more chronic, less chronic.
They were recruited in different ways, and that's really an easy explanation of why things change. Natural history changes. People's health problems are different, and I actually think that the Stone's meta analysis with 70,033 patients says it very clearly. It's a flat line from 1979. And the more data you have, the more you have to believe it. That's all. That's my personal opinion. And I think we actually are very deeply influenced by the media. I mean, I can't believe this:
The mystery of the placebo. We know more about placebo effects at least compared to many drugs on the market. Thanks my opinion. Thanks, Winfried, for letting me say it.
MATTHEW RUDORFER: Thanks, Ted.
We have a question for Greg. The question is, I wonder what the magic of 90 seconds is? Is there a physiologic basis to the turning point when the mouse changes behavior?
GREGORY CORDER: I think I addressed it in a written post somewhere. We don't know. We see a lot of variability in those animals. So like in this putative placebo phase, some mice will remain on that condition side for 40 seconds, 45 seconds, 60 seconds. Or they'll stay there the entire three minutes of the test. We're not exactly sure what's driving the difference in those different animals. These are both male and females. We see the effect in both male and female C57 black six mice, a genetically inbred animal. We always try to restrict the time of day of testing. We do reverse light testing. This is the animal wake cycle.
And there are things like dominance hierarchies within the cages, alpha versus betas. They may have different levels of pain thresholds. But the breaking of whatever the anti nocioceptive effect is they're standing on a hot plate for quite a long time. At some point those nociceptors in the periphery are going to become sensitized and signal. And to some point it's to the animal's advantage to pay attention to pain. You don't want to necessarily go around not paying attention to something that's potentially very dangerous or harmful to you. We would have to scale up the number of animals substantially I think, to really start parse out what the difference is that would account for that. But that's an excellent point, though.
MATTHEW RUDORFER: Carolyn.
CAROLYN RODRIGUEZ: I want to thank all today's speakers and wonderful presentations today. I just wanted to just go back for a second to Dr. Pecina's point about thinking about a placebo effect is not a monolith and also thinking about individual disorders.
And so I'm a clinical trialist and do research in obsessive compulsive disorder, and a lot of the things that are written in the literature meta analysis is that OCD has one of the lowest placebo rates. And so, you know, from what we gathered today, I guess to turn the question on its head is, is why is that, is that the case, why is that the case, and does that say something about OCD pathology, and what about it? Right? How can we really get more refined in terms of different domains and really thinking about the placebo effect.
So just want to say thank you again and to really having a lot of food for thought.
MATTHEW RUDORFER: Thanks. As we're winding down, one of the looming questions on the table remains what are research gaps and where do you think the next set of studies should go. And I think if anyone wants to put some ideas on the table, they'd be welcome.
MICHAEL DETKE: One of the areas that I mentioned in my talk that is hard for industry to study, or there's a big incentive, which is I talked about having third party reviewers review source documents and videos or audios of the HAM D, MADRS, whatever, and that there's not much controlled evidence.
And, you know, it's a fairly simple design, you know, within our largest controlled trial, do this with half the sites and don't do it with the other half.
Blinding isn't perfect. I haven't thought about this, and it can probably be improved upon a lot, but imagine you're the sponsor who's paying the $20 million in three years to run this clinical trial. You want to test your drug as fast as you possibly can. You don't want to really be paying for this methodology.
So that might be -- earlier on Tor or someone mentioned there might be some specific areas where this might be something for NIH to consider picking up. Because that methodology is being used in hundreds of trials, I think, today, the third party remote reviewer. So there's an area to think about.
MATTHEW RUDORFER: Thanks. Holly.
SARAH “HOLLY” LISANBY: Yeah. Carolyn just mentioned one of the gap areas, really trying to understand why some disorders are more amenable to the placebo response than others and what can that teach us. That sounds like a research gap area to me.
Also, throughout these two days we've heard a number of research gap areas having to do with methodology, how to do placebos or shams, how to assess outcome, how to protect the blind, how do you select what your outcome measures should be.
And then also today my mind was going very much towards what can preclinical models teach us and the genetics, the biology of a placebo response, the biogender line, individual differences in placebo response.
There may be clues there. Carolyn, to your point to placebo response being lower in OCD, and yet there are some OCD patients who respond, what's different about them that makes them responders?
And so studies that just look at within a placebo response versus nonresponse or gradation response or durability response and the mechanisms behind that.
These are questions that I think may ultimately facilitate getting drugs and devices to market, but certainly are questions that might be helpful to answer at the research stage, particularly at the translational research stage, in order to inform the design of pivotal trials that you would ultimately do to get things to market.
So it seems like there are many stages before getting to the ideal pivotal trial. So I really appreciate everyone's input. Let me stop talking because I really want to hear what Dr. Hall has to say.
KATHRYN HALL: I wanted to just come back for one of my favorite gaps to this question increasing the placebo effect. I think it's an important one because so many trials are failing these days. And I think it's not all trials are the same.
And what's really fascinating to me is that you see in Phase II clinical trials really great results, and then what's the first thing you do as a pharma company when you got a good result? You get to put out a press release.
And what's the first thing you're going to go do when you enroll in a clinical trial? You're going to read a press release. You're going to read as much as you can about the drug or the trial you're enrolling in. And how placebo boosting is it going to be to see that this trial had amazing effects on this condition you're struggling with.
If lo and behold we go to Phase III, and you can -- we're actually writing a paper on this, how many times we see the words "unexpected results," and I think we saw them here today, today or yesterday. Like, this should not be unexpected. When your Phase III trial fails, you should not be surprised because this is what's happening time and time again.
And I think some of the -- yeah, I agree, Ted, it's like this is a modern time, but there's so much information out there, so much information to sway us towards placebo responses that I think that's a piece of the problem. And finding out what the problem is I think is a really critical gap.
MATTHEW RUDORFER: Winfried.
WINFRIED RIEF: Yeah. May I follow up in that I think it fits quite nicely to what has been said before, and I want to direct I want to answer directly to Michael Detke.
On first glance, it seems less expensive to do the trials the way we do it with one placebo group and one drug arm, and we try to keep the context constant. But this is the problem. We have a constant context without any variation, so we don't learn under which context conditions is this drug really effective and what are the context conditions the drug might not be effective at all.
And therefore I think the current strategy is more like a lottery. It's really by chance it can happen that you are in this little window where the drug can show the most positive effectivity, but it can also be that you are in this little window or the big window where the drug is not able to show its effectivity.
And therefore I think, on second glance, it's a very expensive strategy only to use one single context to evaluate a drug.
MATTHEW RUDORFER: If I have time for--
TED KAPTCHUK: Marta speak, and then Liane should speak.
MARTA PECINA: I just wanted to add kind of a minor comment here, which is this idea that we're going to have to move on from the idea that giving someone a placebo is enough to induce positive expectancies and the fact that expectancies evolve over time.
So at least in some of the data that we've shown, and it's a small sample, but still we see that 50% of those subjects who are given a placebo don't have drug assignment beliefs. And so that is a very large amount of variability there that we are getting confused with everything else.
And so I do think that it is really important, whether in clinical trials, in research, to really come up with very and really develop new ways of measuring expectancies and allow expectancies to be measured over time. Because they do change. We have some prior expectancies, and then we have some expectancies that are learned based on experience. And I do think that this is an area of improvement that the field could improve relatively easily, you know, assess expectancies better, measure expectancies better.
TED KAPTCHUK: Liane, why don't you say something, and Luana, and then Cristina.
LIANE SCHMIDT: So I wanted to -- maybe one -- another open gap is like about the cognition, like what studying placebo, how can it help us to better understand human reasoning, like, and vice versa, actually, all the biases we have, these cognitive processes like motivation, for example, or memory, and yet all the good news about optimism biases, how do they contribute to placebo effects on the patient side but also on the clinician side when the clinicians have to make diagnosis or judge, actually, treatment efficiency based on some clinical scale.
So basically using like tools from cognition, like psychology or cognitive neuroscience, to better understand the processes, the cognitive processes that intervene when we have an expectation and behavior reach out, a symptom or neural activation, what comes in between, like how is it translated, basically, from cognitive predictability.
LUANA COLLOCA: I think we tended to consider expectation as static measurement when in reality we know that what we expect at the beginning of this workshop is slightly different by the end of what we are hearing and, you know, learning.
So expectation is a dynamic phenomenon, and the assumption that we can predict placebo effects with our measurement of expectation can be very limiting in terms of, you know, applications. Rather, it is important to measure expectation over time and also realize that there are so many nuance, like Liane just mentioned, of expectations, you know.
There are people who say I don't expect anything, I try everything, or people who say, oh, I truly want, I will be I truly want to feel better. And these also problematic patients because having an unrealistic expectation can often destroy, as I show, with a violation of expectancies of placebo effects.
TED KAPTCHUK: Are we getting close? Do you want to summarize? Or who's supposed to do that? I don't know.
CRISTINA CUSIN: I think I have a couple of minutes for remarks. There's so much going on, and more questions than answers, of course.
That has been a fantastic symposium, and I was trying to pitch some idea about possibly organizing a summit with all the panelists, all the presenters, and everyone else who wants to join us, because I think that with a coffee or a tea in our hands and talking not through a Zoom video, we could actually come up with some great idea and some collaboration projects.
Anyone who wants to email us, we'll be happy to answer. And we're always open to collaborating and starting a new study, bouncing off each other new ideas. This is what we do for a living. So we're very enthusiastic about people asking difficult questions.
And some of the questions that are ongoing and I think would be future areas is what we were talking a few minutes ago, we don't know if a placebo responder in a migraine study, for example, would be a placebo responder of depression study or IBS study. We don't know if this person is going to be universal placebo responder or is the context include the type of disease they're suffering from so it's going to be fairly different, and why some disorders have lower placebo response rate overall compared to others. Is that a chronicity, a relaxing, remitting disorder, has higher chance of placebo because the system can be modulated, versus a disorder that is considered more chronic and stable? A lot of this information is not known in the natural history.
Also comes to mind the exact trial it is because we almost never have a threshold for number of prior episodes of depression to enter a trial or how chronic has it been or years of depression or other factors that can clearly change our probability of responding to a treatment.
We heard about methodology for clinical trial design and how patients could be responsive to placebo responses or sham, responsive to drug. How about patients who could respond to both? We have no idea how many of those patients are undergoing a trial, universal responders, unless we do a crossover. And we know that crossover is not a popular design for drug trials.
So we need to figure out also aspects of methodology, how to assess outcome, what's the best way to assess the outcome that we want, is it clinically relevant, how to protect the blind aspect, assess expectations and how expectations change over time.
We didn't hear much during the discussion about the role of mindfulness in pain management, and I would like to hear much more about how we're doing in identifying the areas and can we actually intervene on those areas with devices to help with pain management. That's one of the biggest problems we have in terms of clinical care.
In the eating disorder aspect, creating computational models to influence food choices. And, again, with devices or treatments specifically changing the balance about making healthier food choices, I can see an entire field developing. Because most of the medications we prescribe for psychiatric disorders affect food choices and there's weight gain, potentially leading to obesity and cardiovascular complications. So there's an entire field of research we have not touched on.
And the role of animal models in translational results, I don't know if animal researchers, like Greg, talk much with clinical trialists. I think that would be a cross fertilization that is much needed, and we can definitely learn from each other.
And just fantastic. I thank all the panelists for their willingness to work with us and their time, dedication, and just so many meetings to discuss to agree on the program and to divide and conquer different topics. Has been a phenomenal experience, and I'm very, very grateful.
And the NIMH staff has been also amazing, having to collaborate with all of them, and they were so organized. And just a fantastic panel. Thank you, everybody.
MATTHEW RUDORFER: Thank you.
TOR WAGER: Thank you.
NIMH TEAM: Thanks from the NIMH team to all of our participants here.
(Meeting adjourned)
- CBSE Class 10
CBSE Class 10 Maths Competency-Based Questions With Answer Key 2024-25:Chapter 3 Pair of Linear Equations in Two Variables Free PDF Download
Cbse class 10 maths chapter 3 practice questions 2025: cbse class 10 students check and download the competency-focused practice questions for maths chapter 3 pair of linear equations in two variables. .

CBSE 2024-25 Competency Based Questions With Answers: The Central Board of Secondary Education (CBSE) is a national level education body. It has released the competency-based practice questions for students of classes 10 and 12. Students can download them from the school section of Jagran Josh. Here we have given the CBSE Class 10 Maths Chapter 3 Pair of Linear Equations in Two Variables competency-focused questions in pdf format.
The practice questions will be of great help to the students from the point of examinations. It will help cultivate the much needed skills of analysis, critical thinking and problem solving in students. These competency‐based questions are designed specifically to test conceptual understanding and application of concepts. Students can also use it to understand different kinds of questions and practice specific concepts and competencies.
CBSE Class 10 Maths Chapter 3 Competency Based-Questions
| Anjali solved the following equations for the value of x. |
| State true or false for the below statement and justify your answer |
| A pair of linear equations is shown below. |
| The equations of the lines l 1 ,l 2 , and l 3 are given by 5x + 3y = 2p ,35x + 21y = pq , and 100x + 4qy = 240, respectively, where p and q are real numbers. |
| Shown below is a parallelogram with ∠ABC = 70°. |
| Anisha lives 15 km away from her school. She walks to the bus stop and takes a bus to school everyday. |
CBSE Video Courses for Class 10 Students
Class 10 students can study effectively for the exams with the help of video courses prepared by the subject matter experts. These video courses will explain the concepts in a simple and interactive manner which will help learners to understand clearly.
CBSE Class 10 Video Courses
Also, check
CBSE Class 10 Syllabus 2024-25: Download Latest and Revised FREE PDFs
NCERT Books for Class 10 All Subjects PDF (2024-25)
NCERT Solutions for Class 10 (2024-2025) All Subjects & Chapters: Download in PDF
NCERT Rationalised Syllabus Class 10: List of Chapters & Topics Deleted from Books
Polynomial Equations: Concepts, Definition, Formula and Types
Relations and Functions
Profit And Loss
Get here latest School , CBSE and Govt Jobs notification and articles in English and Hindi for Sarkari Naukari , Sarkari Result and Exam Preparation . Download the Jagran Josh Sarkari Naukri App .
- India Post GDS Merit List 2024
- RBI Grade B Admit Card 2024
- UP Police Constable Admit Card 2024
- UGC NET Exam Analysis 2024
- UPSC Calendar 2025
- India GDS Merit List 2024 PDF
- UP Police Exam Analysis 2024 Live Updates
- OPSC OCS Result 2024
- Sri Krishna
- Janmashtami Wishes in Hindi
Latest Education News
Paris Paralympics 2024 India Medal Tally, Check Total Medals Count List
NEET PG Scorecard 2024 Out: NBEMS Releases NEET PG Score Card at nbe.edu.in, Check Details
Who is Manish Narwal? The Golden Boy of Indian Shooting
SSC CGL Tier 1 Admit Card 2024: ssc.nic.in पर जारी, यहाँ से करें टियर-1 परीक्षा के सभी रीजन के एडमिट कार्ड Download
UP NEET UG Counselling 2024: Uttar Pradesh NEET UG Round 1 Seat Allotment Result Anytime Soon at upneet.gov.in
Calcutta University Result 2024 OUT at wbresults.nic.in; Direct Link to Download Semester 6 Marksheet
BEEI Teacher Recruitment 2024: Apply For Teaching Staff Posts, Check Eligibility
SHe-Box Portal: Central Government's Initiative to Ensure Safer Workplaces for Women
Today Current Affairs Hindi One Liners: 30 अगस्त 2024- अवनी लेखरा ने जीता गोल्ड
UP Police Constable Exam Analysis 2024 LIVE: 30 August Shift 1, 2 UPPRPB Paper Review, Difficulty Level
CG SET Answer Key 2024 OUT at vyapam.cgstate.gov.in: Download CG Vyapam Subject Wise Papers
CBSE Class 12 Physics Competency-Based Questions With Answer Key 2024-25: Chapter 5 Atoms and Nuclei FREE PDF Download
CG NEET UG Counselling 2024: Chhattisgarh NEET UG MBBS/BDS Round 1 Seat Allotment Result Out at cgdme.in, Get PDF
MDU Result 2024 OUT on mdu.ac.in; Direct Link to Download UG, PG Marksheet
Madhya Pradesh MP Board Class 12 Subject Wise Syllabus 2024-25: Download Detailed Syllabus PDF!
यूपी पुलिस कांस्टेबल आंसर की 2024: सभी शिफ्टों के लिए UPPRPB अनौपचारिक पेपर PDF यहां से करें डाउनलोड
Today’s School Assembly News Headlines (31th August): Pakistan Invites PM Modi To Attend SCO Meeting In Islamabad In October, PM Modi Lays Foundation For ₹76,200-Crore Vadhvan Port In Maharashtra
Find 3 differences between the girl painting pictures in 19 seconds!
KLEE Result 2024 Date: Kerala 5-year and 3-year LLB Exam Results Soon at cee.kerala.gov.in, Check Qualifying Marks Here
Today Current Affairs Quiz In Hindi: 30 अगस्त 2024- पेरिस पैरालंपिक 2024
- Open access
- Published: 23 August 2024
The role of emotions in academic performance of undergraduate medical students: a narrative review
- Nora Alshareef 1 , 2 ,
- Ian Fletcher 2 &
- Sabir Giga 2
BMC Medical Education volume 24 , Article number: 907 ( 2024 ) Cite this article
225 Accesses
Metrics details
This paper is devoted to a narrative review of the literature on emotions and academic performance in medicine. The review aims to examine the role emotions play in the academic performance of undergraduate medical students.
Eight electronic databases were used to search the literature from 2013 to 2023, including Academic Search Ultimate, British Education Index, CINAHL, Education Abstract, ERIC, Medline, APA Psych Articles and APA Psych Info. Using specific keywords and terms in the databases, 3,285,208 articles were found. After applying the predefined exclusion and inclusion criteria to include only medical students and academic performance as an outcome, 45 articles remained, and two reviewers assessed the quality of the retrieved literature; 17 articles were selected for the narrative synthesis.
The findings indicate that depression and anxiety are the most frequently reported variables in the reviewed literature, and they have negative and positive impacts on the academic performance of medical students. The included literature also reported that a high number of medical students experienced test anxiety during their study, which affected their academic performance. Positive emotions lead to positive academic outcomes and vice versa. However, Feelings of shame did not have any effect on the academic performance of medical students.
The review suggests a significant relationship between emotions and academic performance among undergraduate medical students. While the evidence may not establish causation, it underscores the importance of considering emotional factors in understanding student performance. However, reliance on cross-sectional studies and self-reported data may introduce recall bias. Future research should concentrate on developing anxiety reduction strategies and enhancing mental well-being to improve academic performance.
Peer Review reports
Introduction
Studying medicine is a multi-dimensional process involving acquiring medical knowledge, clinical skills, and professional attitudes. Previous research has found that emotions play a significant role in this process [ 1 , 2 ]. Different types of emotions are important in an academic context, influencing performance on assessments and evaluations, reception of feedback, exam scores, and overall satisfaction with the learning experience [ 3 ]. In particular, medical students experience a wide range of emotions due to many emotionally challenging situations, such as experiencing a heavy academic workload, being in the highly competitive field of medicine, retaining a large amount of information, keeping track of a busy schedule, taking difficult exams, and dealing with a fear of failure [ 4 , 5 , 6 ].Especially during their clinical years, medical students may experience anxiety when interacting with patients who are suffering, ill, or dying, and they must work with other healthcare professionals. Therefore, it is necessary to understand the impact of emotions on medical students to improve their academic outcomes [ 7 ].
To distinguish the emotions frequently experienced by medical students, it is essential to define them. Depression is defined by enduring emotions of sadness, despair, and a diminished capacity for enjoyment or engagement in almost all activities [ 4 ]. Negative emotions encompass unpleasant feelings such as anger, fear, sadness, and anxiety, and they frequently cause distress [ 8 ]. Anxiety is a general term that refers to a state of heightened nervousness or worry, which can be triggered by various factors. Test anxiety, on the other hand, is a specific type of anxiety that arises in the context of taking exams or assessments. Test anxiety is characterised by physiological arousal, negative self-perception, and a fear of failure, which can significantly impair a student’s ability to perform well academically [ 9 , 10 ]. Shame is a self-conscious emotion that arises from the perception of having failed to meet personal or societal standards. It can lead to feelings of worthlessness and inadequacy, severely impacting a student’s motivation and academic performance [ 11 , 12 ]. In contrast, positive emotions indicate a state of enjoyable involvement with the surroundings, encompassing feelings of happiness, appreciation, satisfaction, and love [ 8 ].
Academic performance generally refers to the outcomes of a student’s learning activities, often measured through grades, scores, and other formal assessments. Academic achievement encompasses a broader range of accomplishments, including mastery of skills, attainment of knowledge, and the application of learning in practical contexts. While academic performance is often quantifiable, academic achievement includes qualitative aspects of a student’s educational journey [ 13 ].
According to the literature, 11–40% of medical students suffer from stress, depression, and anxiety due to the intensity of medical school, and these negative emotions impact their academic achievement [ 14 , 15 ]. Severe anxiety may impair memory function, decrease concentration, lead to a state of hypervigilance, and interfere with judgment and cognitive function, further affecting academic performance [ 16 ]. However, some studies have suggested that experiencing some level of anxiety has a positive effect and serves as motivation that can improve academic performance [ 16 , 17 ].
Despite the importance of medical students’ emotions and their relation to academic performance, few studies have been conducted in this area. Most of these studies have focused on the prevalence of specific emotions without correlating with medical students’ academic performance. Few systematic reviews have addressed the emotional challenges medical students face. However, there is a lack of comprehensive reviews that discuss the role of emotions and academic outcomes. Therefore, this review aims to fill this gap by exploring the relationship between emotions and the academic performance of medical students.
Aim of the study
This review aims to examine the role emotions play in the academic performance of undergraduate medical students.
A systematic literature search examined the role of emotions in medical students’ academic performance. The search adhered to the concepts of a systematic review, following the criteria of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [ 18 ]. Then, narrative synthesise was done to analyse the retrieved literature and synthesise the results. A systematic literature search and narrative review provide complete coverage and flexibility to explore and understand findings. Systematic search assures rigour and reduces bias, while narrative synthesis allows for flexible integration and interpretation. This balance improves review quality and utility.
Eligibility criteria
Inclusion criteria.
The study’s scope was confined to January 2013 to December 2023, focusing exclusively on undergraduate medical students. The research encompassed articles originating within medical schools worldwide, accepting content from all countries. The criteria included only full-text articles in English published in peer-reviewed journals. Primary research was considered, embracing quantitative and mixed-method research. The selected studies had to explicitly reference academic performance, test results, or GPA as key outcomes to address the research question.
Exclusion criteria
The study excluded individuals beyond the undergraduate medical student demographic, such as students in other health fields and junior doctors. There was no imposed age limit for the student participants. The research specifically focused on articles within medical schools, excluding those from alternative settings. It solely considered full-text articles in English-language peer-reviewed journals. Letters or commentary articles were excluded, and the study did not limit itself to a particular type of research. Qualitative studies were excluded from the review because they did not have the quantitative measures required to answer the review’s aim. This review excluded articles on factors impacting academic performance, those analysing nursing students, and gender differences. The reasons and numbers for excluding articles are shown in Table 1 .
Information sources
Eight electronic databases were used to search the literature. These were the following: Academic Search Ultimate, British Education Index, CINAHL, Education Abstract, ERIC, Medline, APA Psych Articles and APA Psych Info. The databases were chosen from several fields based on relevant topics, including education, academic evaluation and assessment, medical education, psychology, mental health, and medical research. Initially, with the help of a subject librarian, the researcher used all the above databases; the databases were searched with specific keywords and terms, and the terms were divided into the following concepts emotions, academic performance and medical students. Google Scholar, EBSCOhost, and the reference list of the retrieved articles were also used to identify other relevant articles.
Search strategy
This review started with a search of the databases. Eight electronic databases were used to search the literature from 2013 to 2023. Specific keywords and terms were used to search the databases, resulting in 3,285,208 articles. After removing duplicates, letters and commentary, this number was reduced to 1,637 articles. Exclusion and inclusion criteria were then applied, resulting in 45 articles. After two assessors assessed the literature, 17 articles were selected for the review. The search terms are as follows:
Keywords: Emotion, anxiety, stress, empathy, test anxiety, exam anxiety, test stress, exam stress, depression, emotional regulation, test scores, academic performance, grades, GPA, academic achievement, academic success, test result, assessment, undergraduate medical students and undergraduate medical education.
Emotions: TI (Emotion* OR Anxiety OR Stress OR empathy) OR emotion* OR (test anxiety or exam anxiety or test stress or exam stress) OR (depression) OR AB ((Emotion* OR Anxiety OR Stress OR empathy) OR emotion* OR (test anxiety or exam anxiety or test stress or exam stress)) (MH “Emotions”) OR (MH “Emotional Regulation”) DE “EMOTIONS”.
Academic performance: TI (test scores or academic performance or grades or GPA) OR (academic achievement or academic performance or academic success) OR (test result* OR assessment*) OR AB (test scores or academic performance or grades or GPA) OR (academic achievement or academic performance or academic success) OR test result* OR assessment*.
Medical Students: TI (undergraduate medical students OR undergraduate medical education) OR AB (undergraduate medical students OR undergraduate medical education), TI “medical students” OR AB “medical students” DE “Medical Students”.
Selection process
This literature review attempts to gather only peer-reviewed journal articles published in English on undergraduate medical students’ negative and positive emotions and academic performance from January 2013 to December 2023. Their emotions, including depression, anxiety, physiological distress, shame, happiness, joy, and all emotions related to academic performance, were examined in quantitative research and mixed methods.
Moreover, to focus the search, the author specified and defined each keyword using advanced search tools, such as subject headings in the case of the Medline database. The author used ‘MeSH 2023’ as the subject heading, then entered the term ‘Emotion’ and chose all the relevant meanings. This method was applied to most of the keywords.
Studies were included based on predefined criteria related to study design, participants, exposure, outcomes, and study types. Two independent reviewers screened each record, and the report was retrieved. In the screening process, reviewers independently assessed each article against the inclusion criteria, and discrepancies were resolved through consensus during regular team meetings. In cases of persistent disagreement, a third reviewer was consulted. Endnote library program was used for the initial screening phase. This tool was used to identify duplicates, facilitated the independent screening of titles and abstracts and helped to retrieve the full-text articles. The reasons for excluding the articles are presented in Table 1 .
Data collection process
Two independent reviewers extracted data from the eligible studies, with any discrepancies resolved through discussion and consensus. If the two primary reviewers could not agree, a third reviewer served as an arbitrator. For each included study, the following information was extracted and recorded in a standardised database: first author name, publication year, study design, sample characteristics, details of the emotions exposed, outcome measures, and results.
Academic performance as an outcome for medical students was defined to include the following: Exam scores (e.g., midterm, final exams), Clinical assessments (e.g., practical exams, clinical rotations), Overall grade point average (GPA) or any other relevant indicators of academic achievement.
Data were sought for all outcomes, including all measures, time points, and analyses within each outcome domain. In cases where studies reported multiple measures or time points, all relevant data were extracted to provide a comprehensive overview of academic performance. If a study reported outcomes beyond the predefined domains, inclusion criteria were established to determine whether these additional outcomes would be included in the review. This involved assessing relevance to the primary research question and alignment with the predefined outcome domains.
Quality assessment
The quality and risk of bias in included studies were assessed using the National Institute of Health’s (NIH) critical appraisal tool. The tool evaluates studies based on the following domains: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. Two independent reviewers assessed the risk of bias in each included study. Reviewers worked collaboratively to reach a consensus on assessments. Discrepancies were resolved through discussion and consensus. In cases of persistent disagreement, a third reviewer was consulted.
To determine the validity of eligible articles, all the included articles were critically appraised, and all reviewers assessed bias. The validity and reliability of the results were assessed by using objective measurement. Each article was scored out of 14, with 14 indicating high-quality research and 1 indicating low-quality research. High-quality research, according to the NIH (2013), includes a clear and focused research question, defines the study population, features a high participation rate, mentions inclusion and exclusion criteria, uses clear and specific measurements, reports results in detail, lists the confounding factors and lists the implications for the local community. Therefore, an article was scored 14 if it met all criteria of the critical appraisal tool. Based on scoring, each study was classified into one of three quality categories: good, fair or poor. The poorly rated articles mean their findings were unreliable, and they will not be considered, including two articles [ 16 , 19 ]. Seventeen articles were chosen after critical appraisal using the NIH appraisal tool, as shown in Table 2 .
Effect measures
For each outcome examined in the included studies, various effect measures were utilised to quantify the relationship between emotions and academic performance among undergraduate medical students. The effect measures commonly reported across the studies included prevalence rat, correlation coefficients, and mean differences. The reviewer calculated the effect size for the studies that did not report the effect. The choice of effect measure depended on the nature of the outcome variable and the statistical analysis conducted in each study. These measures were used to assess the strength and direction of the association between emotional factors and academic performance.
The synthesis method
The findings of individual studies were summarised to highlight crucial characteristics. Due to the predicted heterogeneity, the synthesis involved pooling effect estimates and using a narrative method. A narrative synthesis approach was employed in the synthesis of this review to assess and interpret the findings from the included studies qualitatively. The narrative synthesis involved a qualitative examination of the content of each study, focusing on identifying common themes. This synthesis was employed to categorise and interpret data, allowing for a nuanced understanding of the synthesis. Themes related to emotions were identified and extracted for synthesis. Control-value theory [ 20 ] was used as an overarching theory, providing a qualitative synthesis of the evidence and contributing to a deeper understanding of the research question. If the retrieved articles include populations other than medical, such as dental students or non-medical students, the synthesis will distinguish between them and summarise the findings of the medical students only, highlighting any differences or similarities.
The Control-Value Theory, formulated by Pekrun (2006), is a conceptual framework that illustrates the relationship between emotions and academic achievement through two fundamental assessments: control and value. Control pertains to the perceived ability of a learner to exert influence over their learning activities and the results they achieve. Value relates to a student’s significance to these actions and results. The theory suggests that students are prone to experiencing good feelings, such as satisfaction and pride when they possess a strong sense of control and importance towards their academic assignments. On the other hand, individuals are prone to encountering adverse emotions (such as fear and embarrassment) when they perceive a lack of control or worth in these particular occupations. These emotions subsequently impact students’ motivation, learning strategies, and, eventually, their academic achievement. The relevance of control-value theory in reviewing medical student emotions and their influence on academic performance is evident for various reasons. This theory offers a complete framework that facilitates comprehending the intricate connection between emotions and academic achievement. It considers positive and negative emotions, providing a comprehensive viewpoint on how emotions might influence learning and performance. The relevance of control and value notions is particularly significant for medical students due to their frequent exposure to high-stakes tests and difficult courses. Gaining insight into the students’ perception of their power over academic assignments and the importance they attach to their medical education might aid in identifying emotional stimuli and devising remedies. Multiple research has confirmed the theory’s assertions, showing the critical influence of control and value evaluations on students’ emotional experiences and academic achievements [ 21 , 22 ].
Data extraction
For this step, a data extraction sheet was developed using the data extraction template provided by the Cochrane Handbook. To ensure the review is evidence-based and bias-free, the Cochrane Handbook strongly suggests that more than one reviewer review the data. Therefore, the main researcher extracted the data from the included studies, and another reviewer checked the included, excluded and extracted data. Any disagreements were resolved via discussion by a third reviewer. The data extraction Table 2 identified all study features, including the author’s name, the year of publication, the method used the aim of the study, the number and description of participants, data collection tools, and study findings.
Finalisation of references and study characteristics
Prisma sheet and the summary of final studies that have been used for the review.
When the keywords and search terms related to emotions, as mentioned above, in the eight databases listed, 3,285,208 articles were retrieved. After using advanced search and subject headings, the number of articles increased to 3,352,371. Similarly, searching for the second keyword, ‘academic performance,’ using all the advanced search tools yielded 8,119,908 articles. Searching for the third keyword, ‘medical students’, yielded 145,757 articles. All terms were searched in article titles and abstracts. After that, the author combined all search terms by using ‘AND’ and applied the time limit from 2013 to 2023; the search narrowed to 2,570 articles. After duplicates, letters and commentary were excluded, the number was reduced to 1,637 articles. After reading the title and abstract to determine relevance to the topic and applying the exclusion and inclusion criteria mentioned above, 45 articles remained; after the quality of the retrieved literature was assessed by two reviewers, 17 articles were selected for the review. The PRISMA flow diagram summarising the same is presented in Fig. 1 . Additionally, One article by Ansari et al. (2018) was selected for the review; it met most inclusion and exclusion criteria except that the outcome measure is cognitive function and not academic performance. Therefore, it was excluded from the review. Figure 1 shows the Prisma flow diagram (2020) of studies identified from the databases.

Prisma flow diagram (2020)
Study characteristics
Table 2 , summarising the characteristics of the included studies, is presented below.
Findings of the study
Country of the study.
Many of the studies were conducted in developing countries, with the majority being conducted in Europe ( n = 4), followed by Pakistan ( n = 2), then Saudi Arabia ( n = 2), and the United States ( n = 2). The rest of the studies were conducted in South America ( n = 1), Morocco ( n = 1), Brazil ( n = 1), Australia ( n = 1), Iran ( n = 1), South Korea ( n = 1) and Bosnia and Herzegovina ( n = 1). No included studies were conducted in the United Kingdom.
Study design
Regarding study design, most of the included articles used a quantitative methodology, including 12 cross-sectional studies. There were two randomised controlled trials, one descriptive correlation study, one cohort study, and only one mixed-method study.
Population and study setting
Regarding population and setting, most of the studies focused on all medical students studying in a medical school setting, from first-year medical students to those in their final year. One study compared medical students with non-medical students; another combined medical students with dental students.
The study aims varied across the included studies. Seven studies examined the prevalence of depression and anxiety among medical students and their relation to academic performance. Four studies examined the relationship between test anxiety and academic performance in medical education. Four studies examined the relationship between medical students’ emotions and academic achievements. One study explored the influence of shame on medical students’ learning.
Study quality
The studies were assessed for quality using tools created by the NIH (2013) and then divided into good, fair, and poor based on these results. Nine studies had a high-quality methodology, seven achieved fair ratings, and only three achieved poor ratings. The studies that were assigned the poor rating were mainly cross-sectional studies, and the areas of weakness were due to the study design, low response rate, inadequate reporting of the methodology and statistics, invalid tools, and unclear research goals.
Outcome measures
Most of the outcome measures were heterogenous and self-administered questionnaires; one study used focus groups and observation ward assessment [ 23 ]. All the studies used the medical students’ academic grades.
Results of the study
The prevalence rate of psychological distress in the retrieved articles.
Depression and anxiety are the most common forms of psychological distress examined concerning academic outcomes among medical students. Studies consistently show concerningly high rates, with prevalence estimates ranging from 7.3 to 66.4% for anxiety and 3.7–69% for depression. These findings indicate psychological distress levels characterised as moderate to high based on common cut-off thresholds have a clear detrimental impact on academic achievement [ 16 , 24 , 25 , 26 ].
The studies collectively examine the impact of psychological factors on academic performance in medical education contexts, using a range of effect sizes to quantify their findings. Aboalshamat et al. (2015) identified a small effect size ( η 2 = 0.018) for depression’s impact on academic performance, suggesting a modest influence. Mihailescu (2016) found a significant negative correlation between levels of depression/anxiety (rho=-0.14, rho=-0.19), academic performance and GPA among medical students. Burr and Beck Dallaghan (2019) reported professional efficacy explaining 31.3% of the variance in academic performance, indicating a significant effect size. However, Del-Ben (2013) et al. did not provide the significant impact of affective changes on academic achievement, suggesting trivial effect sizes for these factors.
In conclusion, anxiety and depression, both indicators of psychological discomfort, are common among medical students. There is a link between distress and poor academic performance results, implying that this relationship merits consideration. Table 3 below shows the specific value of depression and anxiety in retrieved articles.
Test anxiety
In this review, four studies examined the relationship between test anxiety and academic performance in medical education [ 27 , 28 , 29 , 30 ]. The studies found high rates of test anxiety among medical students, ranging from 52% [ 27 ] to as high as 81.1% [ 29 ]. Final-year students tend to experience the highest test anxiety [ 29 ].
Test anxiety has a significant negative correlation with academic performance measures and grade point average (GPA) [ 27 , 28 , 29 ]. Green et al. (2016) found that test anxiety was moderately negatively correlated with USMLE score ( r = − 0.24, p = 0.00); high test anxiety was associated with low USMLE scores in the control group, further suggesting that anxiety can adversely affect performance. The findings that a test-taking strategy course reduced anxiety without improving test scores highlight the complex nature of anxiety’s impact on performance.
Nazir et al. (2021) found that excellent female medical students reported significantly lower test anxiety than those with low academic grades, with an odds ratio of 1.47, indicating that students with higher test anxiety are more likely to have lower academic grades. Kim’s (2016) research shows moderate correlations between test anxiety and negative achievement emotions such as anxiety and boredom, but interestingly, this anxiety does not significantly affect practical exam scores (OSCE) or GPAs. However, one study found that examination stress enhanced academic performance with a large effect size (W = 0.78), with stress levels at 47.4% among their sample, suggesting that a certain stress level before exams may be beneficial [ 30 ].
Three papers explored shame’s effect on medical students’ academic achievement [ 24 , 31 , 32 ]. Hayat et al. (2018) reported that academic feelings, like shame, significantly depend on the academic year. shame was found to have a slight negative and significant correlation with the academic achievement of learners ( r =-0.15). One study found that some medical students felt shame during simulations-based education examinations because they had made incorrect decisions, which decreased their self-esteem and motivation to learn. However, others who felt shame were motivated to study harder to avoid repeating the same mistakes [ 23 ].
Hautz (2017) study examined how shame affects medical students’ learning using a randomised controlled trial where researchers divided the students into two groups: one group performed a breast examination on mannequins and the other group on actual patients. The results showed that students who performed the clinical examination on actual patients experienced significantly higher levels of shame but performed better in examinations than in the mannequin group. In the final assessments on standardised patients, both groups performed equally well. Therefore, shame decreased with more clinical practice, but shame did not have significant statistics related to learning or performance. Similarly, Burr and Dallaghan (2019) reported that the shame level of medical students was (40%) but had no association with academic performance.
Academic performance, emotions and medical students
Three articles discussed medical students’ emotions and academic performance [ 23 , 24 , 32 ]. Burr and Dallaghan (2019) examine the relationship between academic success and emotions in medical students, such as pride, hope, worry, and shame. It emphasises the links between academic accomplishment and professional efficacy, as well as hope, pride, worry, and shame. Professional efficacy was the most significant factor linked to academic performance, explaining 31.3% of the variance. The importance of emotions on understanding, processing of data, recall of memories, and cognitive burden is emphasised throughout the research. To improve academic achievement, efforts should be made to increase student self-efficacy.
Hayat et al. (2018) found that positive emotions and intrinsic motivation are highly connected with academic achievement, although emotions fluctuate between educational levels but not between genders. The correlations between negative emotions and academic achievement, ranging from − 0.15 to -0.24 for different emotions, suggest small but statistically significant adverse effects.
Behren et al.‘s (2019) mixed-method study found that students felt various emotions during the simulation, focusing on positive emotions and moderate anxiety. However, no significant relationships were found between positive emotions and the student’s performance during the simulation [ 23 ].
This review aims to investigate the role of emotions in the academic performance of undergraduate medical students. Meta-analysis cannot be used because of the heterogeneity of the data collection tools and different research designs [ 33 ]. Therefore, narrative synthesis was adopted in this paper. The studies are grouped into four categories as follows: (1) The effect of depression and anxiety on academic performance, (2) Test anxiety and academic achievement, (3) Shame and academic performance, and (4) Academic performance, emotions and medical students. The control-value theory [ 20 ], will be used to interpret the findings.
The effect of depression and anxiety on academic performance
According to the retrieved research, depression and anxiety can have both a negative and a positive impact on the academic performance of medical students. Severe anxiety may impair memory function, decrease concentration, lead to a state of hypervigilance, interfere with judgment and cognitive function, and further affect academic performance [ 4 ]. Most of the good-quality retrieved articles found that anxiety and depression were associated with low academic performance [ 16 , 24 , 25 , 26 ]. Moreira (2018) and Mihailescu (2016) found that higher depression levels were associated with more failed courses and a lower GPA. However, they did not find any association between anxiety level and academic performance.
By contrast, some studies have suggested that experiencing some level of anxiety reinforces students’ motivation to improve their academic performance [ 16 , 34 ]. Zalihic et al. (2017) conducted a study to investigate anxiety sensitivity about academic success and noticed a positive relationship between anxiety level and high academic scores; they justified this because when medical students feel anxious, they tend to prepare and study more, and they desire to achieve better scores and fulfil social expectations. Similarly, another study found anxiety has a negative impact on academic performance when excessive and a positive effect when manageable, in which case it encourages medical students and motivates them to achieve higher scores [ 35 ].
In the broader literature, the impact of anxiety on academic performance has contradictory research findings. While some studies suggest that having some level of anxiety can boost students’ motivation to improve their academic performance, other research has shown that anxiety has a negative impact on their academic success [ 36 , 37 ]. In the cultural context, education and anxiety attitudes differ widely across cultures. High academic pressure and societal expectations might worsen anxiety in many East Asian societies. Education is highly valued in these societies, frequently leading to significant academic stress. This pressure encompasses attaining high academic marks and outperformance in competitive examinations. The academic demands exerted on students can result in heightened levels of anxiety. The apprehension of not meeting expectations can lead to considerable psychological distress and anxiety, which can appear in their physical and mental health and academic achievement [ 38 , 39 ].
Test anxiety and academic achievement
The majority of the studies reviewed confirm that test anxiety negatively affects academic performance [ 27 , 28 , 29 ]. Several studies have found a significant correlation between test anxiety and academic achievement, indicating that higher levels of test anxiety are associated with lower exam scores and lower academic performance [ 40 , 41 ]. For example, Green et al. (2016) RCT study found that test anxiety has a moderately significant negative correlation with the USMLE score. They found that medical students who took the test-taking strategy course had lower levels of test anxiety than the control group, and their test anxiety scores after the exam had improved from the baseline. Although their test anxiety improved after taking the course, there was no significant difference in the exam scores between students who had and had not taken the course. Therefore, the intervention they used was not effective. According to the control-value theory, this intervention can be improved if they design an emotionally effective learning environment, have a straightforward instructional design, foster self-regulation of negative emotions, and teach students emotion-oriented regulation [ 22 ].
Additionally, according to this theory, students who perceive exams as difficult are more likely to experience test anxiety because test anxiety results from a student’s negative appraisal of the task and outcome values, leading to a reduction in their performance. This aligns with Kim’s (2016) study, which found that students who believed that the OSCE was a problematic exam experienced test anxiety more than other students [ 9 , 22 , 42 ].
In the wider literature, a meta-analysis review by von der Embse (2018) found a medium significant negative correlation ( r =-0.24) between test anxiety and test performance in undergraduate educational settings [ 43 ] . Also, they found a small significant negative correlation ( r =-0.17) between test anxiety and GPA. This indicates that higher levels of test anxiety are associated with lower test performance. Moreover, Song et al. (2021) experimental study examined the effects of test anxiety on working memory capacity and found that test anxiety negatively correlated with academic performance [ 44 ]. Therefore, the evidence from Song’s study suggests a small but significant effect of anxiety on working memory capacity. However, another cross-sectional study revealed that test anxiety in medical students had no significant effect on exam performance [ 45 ]. The complexities of this relationship necessitate additional investigation. Since the retrieved articles are from different countries, it is critical to recognise the possible impact of cultural differences on the impact of test anxiety. Cultural factors such as different educational systems, assessment tools and societal expectations may lead to variances in test anxiety experience and expression across diverse communities [ 46 , 47 ]. Culture has a substantial impact on how test anxiety is expressed and evaluated. Research suggests that the degree and manifestations of test anxiety differ among different cultural settings, emphasising the importance of using culturally validated methods to evaluate test anxiety accurately. A study conducted by Lowe (2019) with Canadian and U.S. college students demonstrated cultural variations in the factors contributing to test anxiety. Canadian students exhibited elevated levels of physiological hyperarousal, but U.S. students had more pronounced cognitive interference. These variations indicate that the cultural environment has an influence on how students perceive and respond to test anxiety, resulting in differing effects on their academic performance in different cultures. Furthermore, scholars highlight the significance of carrying out meticulous instruments to assess test anxiety, which are comparable among diverse cultural cohorts. This technique guarantees that the explanations of test scores are reliable and can be compared across different populations. Hence, it is imperative to comprehend and tackle cultural disparities in order to create efficient interventions and assistance for students who encounter test anxiety in diverse cultural environments. Therefore, there is a need for further studies to examine the level of test anxiety and cultural context.
Shame and academic performance
The review examined three studies that discuss the impact of feelings of shame on academic performance [ 23 , 24 , 48 ]. Generally, shame is considered a negative emotion which involves self-reflection and self-evaluation, and it leads to rumination and self-condemnation [ 49 ]. Intimate examinations conducted by medical students can induce feelings of shame, affecting their ability to communicate with patients and their clinical decisions. Shame can increase the avoidance of intimate physical examinations and also encourage clinical practice [ 23 , 24 , 48 ].
One study found that some medical students felt shame during simulations-based education examinations because they had made incorrect decisions, which decreased their self-esteem and motivation to learn. However, others who felt shame were motivated to study harder to avoid repeating the same mistakes [ 23 ]. Shame decreased with more clinical practice, but shame did not affect their learning or performance [ 48 ]. The literature on how shame affects medical students’ learning is inconclusive [ 31 ].
In the broader literature, shame is considered maladaptive, leading to dysfunctional behaviour, encouraging withdrawal and avoidance of events and inhibiting social interaction. However, few studies have been conducted on shame in the medical field. Therefore, more research is needed to investigate the role of shame in medical students’ academic performance [ 49 ]. In the literature, there are several solutions that can be used to tackle the problem of shame in medical education; it is necessary to establish nurturing learning settings that encourage students to openly discuss their problems and mistakes without the worry of facing severe criticism. This can be accomplished by encouraging medical students to participate in reflective practice, facilitating the processing of their emotions, and enabling them to derive valuable insights from their experiences, all while avoiding excessive self-blame [ 50 ]. Offering robust mentorship and support mechanisms can assist students in effectively managing the difficulties associated with intimate examinations. Teaching staff have the ability to demonstrate proper behaviours and provide valuable feedback and effective mentoring [ 51 ]. Training and workshops that specifically target communication skills and the handling of sensitive situations can effectively equip students to handle intimate tests, hence decreasing the chances of them avoiding such examinations due to feelings of shame [ 52 ].
The literature review focused on three studies that examined the relationship between emotions and the academic achievements of medical students [ 23 , 24 , 32 ].
Behren et al. (2019) mixed-method study on the achievement emotions of medical students during simulations found that placing students in challenging clinical cases that they can handle raises positive emotions. Students perceived these challenges as a positive drive for learning and mild anxiety was considered beneficial. However, the study also found non-significant correlations between emotions and performance during the simulation, indicating a complex relationship between emotions and academic performance. The results revealed that feelings of frustration were perceived to reduce students’ interest and motivation for studying, hampered their decision-making process, and negatively affected their self-esteem, which is consistent with the academic achievement emotions literature where negative emotions are associated with poor intrinsic motivation and reduced the ability to learn [ 3 ].
The study also emphasises that mild anxiety can have positive effects, corroborated by Gregor (2005), which posits that moderate degrees of anxiety can improve performance. The author suggests that an ideal state of arousal (which may be experienced as anxiety) enhances performance. Mild anxiety is commonly seen as a type of psychological stimulation that readies the body for upcoming challenges, frequently referred to as a “fight or flight” response. Within the realm of academic performance, this state of heightened arousal can enhance concentration and optimise cognitive functions such as memory, problem-solving skills, and overall performance. However, once the ideal point is surpassed, any additional increase in arousal can result in a decline in performance [ 53 ]. This is additionally supported by Cassady and Johnson (2002), who discovered that a specific level of anxiety can motivate students to engage in more comprehensive preparation, hence enhancing their performance.
The reviewed research reveals a positive correlation between positive emotions and academic performance and a negative correlation between negative emotions and academic performance. These findings align with the control–value theory [ 8 , 22 ], which suggests that positive emotions facilitate learning through mediating factors, including cognitive learning strategies such as strategic thinking, critical thinking and problem-solving and metacognitive learning strategies such as monitoring, regulating, and planning students’ intrinsic and extrinsic motivation. Additionally, several studies found that extrinsic motivation from the educational environment and the application of cognitive and emotional strategies improve students’ ability to learn and, consequently, their academic performance [ 23 , 24 , 32 ]. By contrast, negative emotions negatively affect academic performance. This is because negative emotions reduce students’ motivation, concentration, and ability to process information [ 23 , 24 , 32 ].
Limitations of the study
This review aims to thoroughly investigate the relationship between emotions and academic performance in undergraduate medical students, but it has inherent limitations. Overall, the methodological quality of the retrieved studies is primarily good and fair. Poor-quality research was excluded from the synthesis. The good-quality papers demonstrated strengths in sampling techniques, data analysis, collection and reporting. However, most of the retrieved articles used cross-section studies, and the drawback of this is a need for a more causal relationship, which is a limitation in the design of cross-sectional studies. Furthermore, given the reliance on self-reported data, there were concerns about potential recall bias. These methodological difficulties were noted in most of the examined research. When contemplating the implications for practice and future study, the impact of these limitations on the validity of the data should be acknowledged.
The limitation of the review process and the inclusion criteria restricted the study to articles published from January 2013 to December 2023, potentially overlooking relevant research conducted beyond this timeframe. Additionally, the exclusive focus on undergraduate medical students may constrain the applicability of findings to other health fields or educational levels.
Moreover, excluding articles in non-English language and those not published in peer-reviewed journals introduces potential language and publication biases. Reliance on electronic databases and specific keywords may inadvertently omit studies using different terms or indexing. While the search strategy is meticulous, it might not cover every relevant study due to indexing and database coverage variations. However, the two assessors’ involvement in study screening, selection, data extraction, and quality assessment improved the robustness of the review and ensured that it included all the relevant research.
In conclusion, these limitations highlight the need for careful interpretation of the study’s findings and stress the importance of future research addressing these constraints to offer a more comprehensive understanding of the nuanced relationship between emotions and academic performance in undergraduate medical education.
Conclusion and future research
The review exposes the widespread prevalence of depression, anxiety and test anxiety within the medical student population. The impact on academic performance is intricate, showcasing evidence of adverse and favourable relationships. Addressing the mental health challenges of medical students necessitates tailored interventions for enhancing mental well-being in medical education. Furthermore, it is crucial to create practical strategies considering the complex elements of overcoming test anxiety. Future research should prioritise the advancement of anxiety reduction strategies to enhance academic performance, focusing on the control-value theory’s emphasis on creating an emotionally supportive learning environment. Additionally, Test anxiety is very common among medical students, but the literature has not conclusively determined its actual effect on academic performance. Therefore, there is a clear need for a study that examines the relationship between test anxiety and academic performance. Moreover, the retrieved literature did not provide effective solutions for managing test anxiety. This gap highlights the need for practical solutions informed by Pekrun’s Control-Value Theory. Ideally, a longitudinal study measuring test anxiety and exam scores over time would be the most appropriate approach. it is also necessary to explore cultural differences to develop more effective solutions and support systems tailored to specific cultural contexts.
The impact of shame on academic performance in medical students was inconclusive. Shame is a negative emotion that has an intricate influence on learning outcomes. The inadequacy of current literature emphasises the imperative for additional research to unravel the nuanced role of shame in the academic journeys of medical students.
Overall, emotions play a crucial role in shaping students’ academic performance, and research has attempted to find solutions to improve medical students’ learning experiences; thus, it is recommended that medical schools revise their curricula and consider using simulation-based learning in their instructional designs to enhance learning and improve students’ emotions. Also, studies have suggested using academic coaching to help students achieve their goals, change their learning styles, and apply self-testing and simple rehearsal of the material. Moreover, the study recommended to improve medical students’ critical thinking and autonomy and changing teaching styles to support students better.
Data availability
all included articles are mentioned in the manuscript, The quality assessment of included articles are located in the supplementary materials file no. 1.
Weurlander M, Lonn A, Seeberger A, Hult H, Thornberg R, Wernerson A. Emotional challenges of medical students generate feelings of uncertainty. Med Educ. 2019;53(10):1037–48.
Article Google Scholar
Boekaerts M, Pekrun R. Emotions and emotion regulation in academic settings. Handbook of educational psychology: Routledge; 2015. pp. 90–104.
Google Scholar
Camacho-Morles J, Slemp GR, Pekrun R, Loderer K, Hou H, Oades LG. Activity achievement emotions and academic performance: a meta-analysis. Educational Psychol Rev. 2021;33(3):1051–95.
Aboalshamat K, Hou X-Y, Strodl E. Psychological well-being status among medical and dental students in Makkah, Saudi Arabia: a cross-sectional study. Med Teach. 2015;37(Suppl 1):S75–81.
Mirghni HO, Ahmed Elnour MA. The perceived stress and approach to learning effects on academic performance among Sudanese medical students. Electron Physician. 2017;9(4):4072–6.
Baessler F, Zafar A, Schweizer S, Ciprianidis A, Sander A, Preussler S, et al. Are we preparing future doctors to deal with emotionally challenging situations? Analysis of a medical curriculum. Patient Educ Couns. 2019;102(7):1304–12.
Rowe AD, Fitness J. Understanding the role of negative emotions in Adult Learning and Achievement: a Social Functional Perspective. Behav Sci (Basel). 2018;8(2).
Pekrun R, Frenzel AC, Goetz T, Perry RP. The control-value theory of achievement emotions: An integrative approach to emotions in education. Emotion in education: Elsevier; 2007. pp. 13–36.
Zeidner M. Test anxiety: The state of the art. 1998.
Cassady JC, Johnson RE. Cognitive test anxiety and academic performance. Contemp Educ Psychol. 2002;27(2):270–95.
Tangney JP, Dearing RL. Shame and guilt: Guilford Press; 2003.
Fang J, Brown GT, Hamilton R. Changes in Chinese students’ academic emotions after examinations: pride in success, shame in failure, and self-loathing in comparison. Br J Educ Psychol. 2023;93(1):245–61.
York TT, Gibson C, Rankin S. Defining and measuring academic success. Practical Assess Res Evaluation. 2019;20(1):5.
Abdulghani HM, Irshad M, Al Zunitan MA, Al Sulihem AA, Al Dehaim MA, Al Esefir WA, et al. Prevalence of stress in junior doctors during their internship training: a cross-sectional study of three Saudi medical colleges’ hospitals. Neuropsychiatr Dis Treat. 2014;10:1879–86.
Moreira de Sousa J, Moreira CA, Telles-Correia D, Anxiety. Depression and academic performance: a Study Amongst Portuguese Medical Students Versus non-medical students. Acta Med Port. 2018;31(9):454–62.
Junaid MA, Auf AI, Shaikh K, Khan N, Abdelrahim SA. Correlation between academic performance and anxiety in Medical students of Majmaah University - KSA. JPMA J Pakistan Med Association. 2020;70(5):865–8.
MihĂIlescu AI, Diaconescu LV, Donisan T, Ciobanu AM, THE INFLUENCE OF EMOTIONAL, DISTRESS ON THE ACADEMIC PERFORMANCE IN UNDERGRADUATE MEDICAL STUDENTS. Romanian J Child Adolesc Psychiatry. 2016;4(1/2):27–40.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372.
Hahn H, Kropp P, Kirschstein T, Rücker G, Müller-Hilke B. Test anxiety in medical school is unrelated to academic performance but correlates with an effort/reward imbalance. PLoS ONE. 2017;12(2):1–13.
Pekrun R. The control-value theory of achievement emotions: assumptions, corollaries, and Implications for Educational Research and Practice. Educational Psychol Rev. 2006;18(4):315–41.
Graesser AC. Emotions are the experiential glue of learning environments in the 21st century. Learn Instruction. 2019.
Pekrun R, Perry RP. Control-value theory of achievement emotions. International handbook of emotions in education: Routledge; 2014. pp. 120 – 41.
Behrens CC, Dolmans DH, Gormley GJ, Driessen EW. Exploring undergraduate students achievement emotions during ward round simulation: a mixed-method study. BMC Med Educ. 2019;19(1):316.
Burr J, Beck-Dallaghan GL. The relationship of emotions and Burnout to Medical Students’ academic performance. Teach Learn Med. 2019;31(5):479–86.
Zalihić A, Mešukić S, Sušac B, Knezović K, Martinac M. Anxiety sensitivity as a predictor of academic success of medical students at the University of Mostar. Psychiatria Danubina. 2017;29(Suppl 4):851–4.
Del-Ben CM, Machado VF, Madisson MM, Resende TL, Valério FP, Troncon LEDA. Relationship between academic performance and affective changes during the first year at medical school. Med Teach. 2013;35(5):404–10.
Nazir MA, Izhar F, Talal A, Sohail ZB, Majeed A, Almas K. A quantitative study of test anxiety and its influencing factors among medical and dental students. J Taibah Univ Med Sci. 2021;16(2):253–9.
Green M, Angoff N, Encandela J. Test anxiety and United States Medical Licensing Examination scores. Clin Teacher. 2016;13(2):142–6.
Ben Loubir D, Serhier Z, Diouny S, Battas O, Agoub M, Bennani Othmani M. Prevalence of stress in Casablanca medical students: a cross-sectional study. Pan Afr Med J. 2014;19:149.
Kausar U, Haider SI, Mughal IA, Noor MSA, Stress levels; stress levels of final year mbbs students and its effect on their academic performance. Prof Med J. 2018;25(6):932–6.
Hautz WE, Schröder T, Dannenberg KA, März M, Hölzer H, Ahlers O, et al. Shame in Medical Education: a randomized study of the Acquisition of intimate Examination skills and its effect on subsequent performance. Teach Learn Med. 2017;29(2):196–206.
Hayat AA, Salehi A, Kojuri J. Medical student’s academic performance: the role of academic emotions and motivation. J Adv Med Educ Professionalism. 2018;6(4):168–75.
Deeks JJ, Riley RD, Higgins JP. Combining Results Using Meta-Analysis. Systematic Reviews in Health Research: Meta‐Analysis in Context. 2022:159 – 84.
Aboalshamat K, Hou X-Y, Strodl E. The impact of a self-development coaching programme on medical and dental students’ psychological health and academic performance: a randomised controlled trial. BMC Med Educ. 2015;15:134.
Jamil H, Alakkari M, Al-Mahini MS, Alsayid M, Al Jandali O. The impact of anxiety and depression on academic performance: a cross-sectional study among medical students in Syria. Avicenna J Med. 2022;12(03):111–9.
Mirawdali S, Morrissey H, Ball P. Academic anxiety and its effects on academic performance. 2018.
Al-Qaisy LM. The relation of depression and anxiety in academic achievement among group of university students. Int J Psychol Couns. 2011;3(5):96–100.
Cheng DR, Poon F, Nguyen TT, Woodman RJ, Parker JD. Stigma and perception of psychological distress and depression in Australian-trained medical students: results from an inter-state medical school survey. Psychiatry Res. 2013;209(3):684–90.
Lee M, Larson R. The Korean ‘examination hell’: long hours of studying, distress, and depression. J Youth Adolesc. 2000;29(2):249–71.
Ali SK. 861 – Social phobia among medical students. Eur Psychiatry. 2013;28:1.
Bonna AS, Sarwar M, Md Nasrullah A, Bin Razzak S, Chowdhury KS, Rahman SR. Exam anxiety among medical students in Dhaka City and its Associated Factors-A cross-sectional study. Asian J Med Health. 2022;20(11):20–30.
Kim K-J. Factors associated with medical student test anxiety in objective structured clinical examinations: a preliminary study. Int J Med Educ. 2016;7:424–7.
Von der Embse N, Jester D, Roy D, Post J. Test anxiety effects, predictors, and correlates: a 30-year meta-analytic review. J Affect Disord. 2018;227:483–93.
Song J, Chang L, Zhou R. Test anxiety impairs filtering ability in visual working memory: evidence from event-related potentials. J Affect Disord. 2021;292:700–7.
Theobald M, Breitwieser J, Brod G. Test anxiety does not predict exam performance when knowledge is controlled for: strong evidence against the interference hypothesis of test anxiety. Psychol Sci. 2022;33(12):2073–83.
Lowe PA. Examination of test anxiety in samples of Australian and US Higher Education Students. High Educ Stud. 2019;9(4):33–43.
Kavanagh BE, Ziino SA, Mesagno C. A comparative investigation of test anxiety, coping strategies and perfectionism between Australian and United States students. North Am J Psychol. 2016;18(3).
Mihăilescu AI, Diaconescu LV, Ciobanu AM, Donisan T, Mihailescu C. The impact of anxiety and depression on academic performance in undergraduate medical students. Eur Psychiatry. 2016;33:S341–2.
Terrizzi JA Jr, Shook NJ. On the origin of shame: does shame emerge from an evolved disease-avoidance architecture? Front Behav Neurosci. 2020;14:19.
Epstein RM. Mindful practice. JAMA. 1999;282(9):833–9.
Hauer KE, Teherani A, Dechet A, Aagaard EM. Medical students’ perceptions of mentoring: a focus-group analysis. Med Teach. 2005;27(8):732–4.
Kalet A, Pugnaire MP, Cole-Kelly K, Janicik R, Ferrara E, Schwartz MD, et al. Teaching communication in clinical clerkships: models from the macy initiative in health communications. Acad Med. 2004;79(6):511–20.
Gregor A. Examination anxiety: live with it, control it or make it work for you? School Psychol Int. 2005;26(5):617–35.
Download references
Acknowledgements
I would like to thank Lancaster university library for helping me to search the literature and to find the appropriate databases and thanks to Lancaster university to prove access to several softwares.
No funding.
Author information
Authors and affiliations.
King Abdulaziz University, Jeddah, Saudi Arabia
Nora Alshareef
Lancaster University, Lancaster, UK
Nora Alshareef, Ian Fletcher & Sabir Giga
You can also search for this author in PubMed Google Scholar
Contributions
NA made substantial contributions throughout the systematic review process and was actively involved in writing and revising the manuscript. NA’s responsible for the design of the study, through the acquisition, analysis, and interpretation of data, to the drafting and substantive revision of the manuscript. NA has approved the submitted version and is personally accountable for her contributions, ensuring the accuracy and integrity of the work. IF was instrumental in screening the literature, extracting data, and conducting the quality assessment of the included studies. Additionally, IF played a crucial role in revising the results and discussion sections of the manuscript, ensuring that the interpretation of data was both accurate and insightful. IF has approved the submitted version and has agreed to be personally accountable for his contributions, particularly in terms of the accuracy and integrity of the parts of the work he was directly involved in. SG contributed significantly to the selection of papers and data extraction, demonstrating critical expertise in resolving disagreements among authors. SG’s involvement was crucial in revising the entire content of the manuscript, enhancing its coherence and alignment with the study’s objectives. SG has also approved the submitted version and is personally accountable for his contributions, committed to upholding the integrity of the entire work.
Corresponding author
Correspondence to Nora Alshareef .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
Consent of publication was obtained from the other authors.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/ .
Reprints and permissions
About this article
Cite this article.
Alshareef, N., Fletcher, I. & Giga, S. The role of emotions in academic performance of undergraduate medical students: a narrative review. BMC Med Educ 24 , 907 (2024). https://doi.org/10.1186/s12909-024-05894-1
Download citation
Received : 08 March 2024
Accepted : 12 August 2024
Published : 23 August 2024
DOI : https://doi.org/10.1186/s12909-024-05894-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Medical students
- Academic performance
BMC Medical Education
ISSN: 1472-6920
- General enquiries: [email protected]
Have a language expert improve your writing
Run a free plagiarism check in 10 minutes, generate accurate citations for free.
- Knowledge Base
Methodology
- Independent vs. Dependent Variables | Definition & Examples
Independent vs. Dependent Variables | Definition & Examples
Published on February 3, 2022 by Pritha Bhandari . Revised on June 22, 2023.
In research, variables are any characteristics that can take on different values, such as height, age, temperature, or test scores.
Researchers often manipulate or measure independent and dependent variables in studies to test cause-and-effect relationships.
- The independent variable is the cause. Its value is independent of other variables in your study.
- The dependent variable is the effect. Its value depends on changes in the independent variable.
Your independent variable is the temperature of the room. You vary the room temperature by making it cooler for half the participants, and warmer for the other half.
Table of contents
What is an independent variable, types of independent variables, what is a dependent variable, identifying independent vs. dependent variables, independent and dependent variables in research, visualizing independent and dependent variables, other interesting articles, frequently asked questions about independent and dependent variables.
An independent variable is the variable you manipulate or vary in an experimental study to explore its effects. It’s called “independent” because it’s not influenced by any other variables in the study.
Independent variables are also called:
- Explanatory variables (they explain an event or outcome)
- Predictor variables (they can be used to predict the value of a dependent variable)
- Right-hand-side variables (they appear on the right-hand side of a regression equation).
These terms are especially used in statistics , where you estimate the extent to which an independent variable change can explain or predict changes in the dependent variable.
Receive feedback on language, structure, and formatting
Professional editors proofread and edit your paper by focusing on:
- Academic style
- Vague sentences
- Style consistency
See an example

There are two main types of independent variables.
- Experimental independent variables can be directly manipulated by researchers.
- Subject variables cannot be manipulated by researchers, but they can be used to group research subjects categorically.
Experimental variables
In experiments, you manipulate independent variables directly to see how they affect your dependent variable. The independent variable is usually applied at different levels to see how the outcomes differ.
You can apply just two levels in order to find out if an independent variable has an effect at all.
You can also apply multiple levels to find out how the independent variable affects the dependent variable.
You have three independent variable levels, and each group gets a different level of treatment.
You randomly assign your patients to one of the three groups:
- A low-dose experimental group
- A high-dose experimental group
- A placebo group (to research a possible placebo effect )

A true experiment requires you to randomly assign different levels of an independent variable to your participants.
Random assignment helps you control participant characteristics, so that they don’t affect your experimental results. This helps you to have confidence that your dependent variable results come solely from the independent variable manipulation.
Subject variables
Subject variables are characteristics that vary across participants, and they can’t be manipulated by researchers. For example, gender identity, ethnicity, race, income, and education are all important subject variables that social researchers treat as independent variables.
It’s not possible to randomly assign these to participants, since these are characteristics of already existing groups. Instead, you can create a research design where you compare the outcomes of groups of participants with characteristics. This is a quasi-experimental design because there’s no random assignment. Note that any research methods that use non-random assignment are at risk for research biases like selection bias and sampling bias .
Your independent variable is a subject variable, namely the gender identity of the participants. You have three groups: men, women and other.
Your dependent variable is the brain activity response to hearing infant cries. You record brain activity with fMRI scans when participants hear infant cries without their awareness.
A dependent variable is the variable that changes as a result of the independent variable manipulation. It’s the outcome you’re interested in measuring, and it “depends” on your independent variable.
In statistics , dependent variables are also called:
- Response variables (they respond to a change in another variable)
- Outcome variables (they represent the outcome you want to measure)
- Left-hand-side variables (they appear on the left-hand side of a regression equation)
The dependent variable is what you record after you’ve manipulated the independent variable. You use this measurement data to check whether and to what extent your independent variable influences the dependent variable by conducting statistical analyses.
Based on your findings, you can estimate the degree to which your independent variable variation drives changes in your dependent variable. You can also predict how much your dependent variable will change as a result of variation in the independent variable.
Distinguishing between independent and dependent variables can be tricky when designing a complex study or reading an academic research paper .
A dependent variable from one study can be the independent variable in another study, so it’s important to pay attention to research design .
Here are some tips for identifying each variable type.
Recognizing independent variables
Use this list of questions to check whether you’re dealing with an independent variable:
- Is the variable manipulated, controlled, or used as a subject grouping method by the researcher?
- Does this variable come before the other variable in time?
- Is the researcher trying to understand whether or how this variable affects another variable?
Recognizing dependent variables
Check whether you’re dealing with a dependent variable:
- Is this variable measured as an outcome of the study?
- Is this variable dependent on another variable in the study?
- Does this variable get measured only after other variables are altered?
Here's why students love Scribbr's proofreading services
Discover proofreading & editing
Independent and dependent variables are generally used in experimental and quasi-experimental research.
Here are some examples of research questions and corresponding independent and dependent variables.
| Research question | Independent variable | Dependent variable(s) |
|---|---|---|
| Do tomatoes grow fastest under fluorescent, incandescent, or natural light? | ||
| What is the effect of intermittent fasting on blood sugar levels? | ||
| Is medical marijuana effective for pain reduction in people with chronic pain? | ||
| To what extent does remote working increase job satisfaction? |
For experimental data, you analyze your results by generating descriptive statistics and visualizing your findings. Then, you select an appropriate statistical test to test your hypothesis .
The type of test is determined by:
- your variable types
- level of measurement
- number of independent variable levels.
You’ll often use t tests or ANOVAs to analyze your data and answer your research questions.
In quantitative research , it’s good practice to use charts or graphs to visualize the results of studies. Generally, the independent variable goes on the x -axis (horizontal) and the dependent variable on the y -axis (vertical).
The type of visualization you use depends on the variable types in your research questions:
- A bar chart is ideal when you have a categorical independent variable.
- A scatter plot or line graph is best when your independent and dependent variables are both quantitative.
To inspect your data, you place your independent variable of treatment level on the x -axis and the dependent variable of blood pressure on the y -axis.
You plot bars for each treatment group before and after the treatment to show the difference in blood pressure.

If you want to know more about statistics , methodology , or research bias , make sure to check out some of our other articles with explanations and examples.
- Normal distribution
- Degrees of freedom
- Null hypothesis
- Discourse analysis
- Control groups
- Mixed methods research
- Non-probability sampling
- Quantitative research
- Ecological validity
Research bias
- Rosenthal effect
- Implicit bias
- Cognitive bias
- Selection bias
- Negativity bias
- Status quo bias
An independent variable is the variable you manipulate, control, or vary in an experimental study to explore its effects. It’s called “independent” because it’s not influenced by any other variables in the study.
A dependent variable is what changes as a result of the independent variable manipulation in experiments . It’s what you’re interested in measuring, and it “depends” on your independent variable.
In statistics, dependent variables are also called:
Determining cause and effect is one of the most important parts of scientific research. It’s essential to know which is the cause – the independent variable – and which is the effect – the dependent variable.
You want to find out how blood sugar levels are affected by drinking diet soda and regular soda, so you conduct an experiment .
- The type of soda – diet or regular – is the independent variable .
- The level of blood sugar that you measure is the dependent variable – it changes depending on the type of soda.
No. The value of a dependent variable depends on an independent variable, so a variable cannot be both independent and dependent at the same time. It must be either the cause or the effect, not both!
Yes, but including more than one of either type requires multiple research questions .
For example, if you are interested in the effect of a diet on health, you can use multiple measures of health: blood sugar, blood pressure, weight, pulse, and many more. Each of these is its own dependent variable with its own research question.
You could also choose to look at the effect of exercise levels as well as diet, or even the additional effect of the two combined. Each of these is a separate independent variable .
To ensure the internal validity of an experiment , you should only change one independent variable at a time.
Cite this Scribbr article
If you want to cite this source, you can copy and paste the citation or click the “Cite this Scribbr article” button to automatically add the citation to our free Citation Generator.
Bhandari, P. (2023, June 22). Independent vs. Dependent Variables | Definition & Examples. Scribbr. Retrieved August 30, 2024, from https://www.scribbr.com/methodology/independent-and-dependent-variables/
Is this article helpful?

Pritha Bhandari
Other students also liked, guide to experimental design | overview, steps, & examples, explanatory and response variables | definitions & examples, confounding variables | definition, examples & controls, what is your plagiarism score.
IMAGES
VIDEO
COMMENTS
The first question asks for a ready-made solution, and is not focused or researchable. The second question is a clearer comparative question, but note that it may not be practically feasible. For a smaller research project or thesis, it could be narrowed down further to focus on the effectiveness of drunk driving laws in just one or two countries.
The quantitative research design that we select subsequently determines whether we look for relationships, associations, trends or interactions. To learn how to structure (i.e., write out) each of these three types of quantitative research question (i.e., descriptive, comparative, relationship-based research questions), see the article: How to ...
INTRODUCTION. Scientific research is usually initiated by posing evidenced-based research questions which are then explicitly restated as hypotheses.1,2 The hypotheses provide directions to guide the study, solutions, explanations, and expected results.3,4 Both research questions and hypotheses are essentially formulated based on conventional theories and real-world processes, which allow the ...
3. Narrow down your topic and determine potential research questions. Once you have gathered enough knowledge on the topic you want to pursue, you can start focusing on a more specific area of study and narrowing down a research question. One option is to focus on gaps in existing knowledge or recent literature.
A good research question is essential to guide your research paper, dissertation, or thesis. All research questions should be: Focused on a single problem or issue. Researchable using primary and/or secondary sources. Feasible to answer within the timeframe and practical constraints. Specific enough to answer thoroughly.
This example research question targets two clearly defined variables, which can be measured and analysed relatively easily. Do online courses result in better retention of material than traditional courses? Timely, specific and focused, answering this research question can help inform educational policy and personal choices about learning formats.
QUALITATIVE RESEARCH QUESTIONS In a qualitative study, inquirers state research questions, not objectives (i.e., specific goals for the research) or hypotheses (i.e., predictions that involve variables and statistical tests). These research questions assume two forms: a central question and associated subquestions.
Variables Cont. • There are three characteristics of variables that are necessary considerations in most research; they are: - A. definition, - B. function, and. - C. type of measurement (i.e., measurement scale) Variables: Definitions. Definitions. • An operational definition "assigns meaning to a construct.
Formulating the research question and hypothesis from existing data (e.g., a database) can lead to multiple statistical comparisons and potentially spurious findings due to chance. ... A relationship-based hypothesis predicts a relationship between two or more variables. It suggests that changes in one variable will correspond to changes in ...
5. Phrase your hypothesis in three ways. To identify the variables, you can write a simple prediction in if…then form. The first part of the sentence states the independent variable and the second part states the dependent variable. If a first-year student starts attending more lectures, then their exam scores will improve.
A research question is a clear, focused, concise, and arguable question on which your research and writing are centered. 1 It states various aspects of the study, including the population and variables to be studied and the problem the study addresses. These questions also set the boundaries of the study, ensuring cohesion.
"A hypothesis is a conjectural statement of the relation between two or more variables". (Kerlinger, 1956) "Hypothesis is a formal statement that presents the expected relationship between an independent and dependent variable."(Creswell, 1994) "A research question is essentially a hypothesis asked in the form of a question."
A comparative research question is a type of quantitative research question that is used to gather information about the differences between two or more research subjects across different variables. These types of questions help the researcher to identify distinct features that mark one research subject from the other while highlighting ...
A confounding variable (also known as a third variable or lurking variable) is an extraneous factor that can influence the relationship between two variables being studied. Specifically, for a variable to be considered a confounding variable, it needs to meet two criteria: It must be correlated with the independent variable (this can be causal ...
Understanding Quantitative Research Questions. Quantitative research involves collecting and analyzing numerical data to answer research questions and test hypotheses. These questions typically seek to understand the relationships between variables, predict outcomes, or compare groups. Let's explore some examples of quantitative research ...
Five Examples of Statistical Research Questions. In writing the statistical research questions, I provide a topic that shows the variables of the study, the study description, and a link to the original scientific article to give you a glimpse of the real-world examples. Topic 1: Physical Fitness and Academic Achievement
Experiments using sounds suggest that we are less responsive during stages 3 and 4 sleep (deep sleep) than during stages 1, 2, or REM sleep (lighter sleep). Thus, the researcher predicts that research participants will be less responsive to odors during stages 3 and 4 sleep than during the other stages of sleep.
Definition: Research questions are the specific questions that guide a research study or inquiry. These questions help to define the scope of the research and provide a clear focus for the study. Research questions are usually developed at the beginning of a research project and are designed to address a particular research problem or objective.
Research questions can be categorized into different types, depending on the type of research to be undertaken. ... Comparative questions are helpful when studying groups with dependent variables where one variable is compared with another. Relationship-based questions try to answer whether or not one variable has an influence on another. These ...
Read More - 90+ Market Research Questions to Ask Your Customers. 1. Select the Type of Quantitative Question. The first step is to determine which type of quantitative question you want to add to your study. There are three types of quantitative questions: Descriptive. Comparative. Relationship-based.
Research questions are used in both qualitative and quantitative research, although what makes a good research question might vary between the two. ... This type of quantitative research question examines how one variable affects another. For example: How does a low level of sunlight affect the mood scores (1-10) of Antarctic explorers during ...
The development of covariational reasoning as a theoretical construct. Covariation necessarily involves at least two magnitudes varying simultaneously: when conceptualizing how a single quantity's values vary, studies in mathematics education refer to it as variational reasoning (Thompson & Carlson, Citation 2017).Several conceptions that emerged in the last decades contributed to a full ...
The National Institute of Mental Health (NIMH) hosted a virtual workshop on the placebo effect. The purpose of this workshop was to bring together experts in neurobiology, clinical trials, and regulatory science to examine placebo effects in drug, device, and psychosocial interventions for mental health conditions. Topics included interpretability of placebo signals within the context of ...
Skills can be categorized into two groups: hard and soft skills. ... The study was guided by the following research question as: ... Results of the t Test of the Differences Between the Average Responses of the Research Sample According to Variable of Type. Dimension Type N Mean t Sig. F; Networking: Male: 147: 36.3469: 1.895.059: 0.666: Female ...
Now that you have gone through the questions, download volume 3 and 4 of CBSE Class 10 Mathematics Chapter 3 Pair of Linear Equations in Two Variables competency-focused practice questions from ...
Example (salt tolerance experiment) Independent variables (aka treatment variables) Variables you manipulate in order to affect the outcome of an experiment. The amount of salt added to each plant's water. Dependent variables (aka response variables) Variables that represent the outcome of the experiment.
Funding for the study was provided in part by the National Science Foundation (grant nos. DEB-1557007, NSF PRFB-1612862 and NSF IOS-1750833), the National Environment Research Council (NE/P003915/1 and NSF IOS-1750833) and the U.S. Air Force Office of Scientific Research (AFOSR MURI award FA9550-22-1-0315).
Medical education was utterly disrupted for two years by the COVID-19 pandemic. In the midst of rearranging courses and adapting to online platforms we, with lecturers and course managers around the globe, wondered what the conversion to online setting did to students' learning, motivation and self-efficacy [1,2,3].What the long-term consequences would be [] and if scalable online medical ...
Studying medicine is a multi-dimensional process involving acquiring medical knowledge, clinical skills, and professional attitudes. Previous research has found that emotions play a significant role in this process [1, 2].Different types of emotions are important in an academic context, influencing performance on assessments and evaluations, reception of feedback, exam scores, and overall ...
The independent variable is the cause. Its value is independent of other variables in your study. The dependent variable is the effect. Its value depends on changes in the independent variable. Example: Independent and dependent variables. You design a study to test whether changes in room temperature have an effect on math test scores.